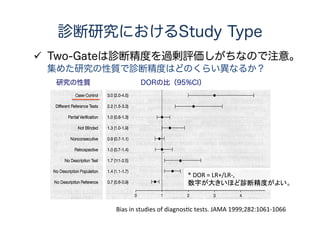
検査・診断の言葉の定義
感度 = ×100(%)
特異度 = × 100(%)
病気あり 病気なし 計
検査異常(陽性) a b a + b
検査正常(陰性) c d c + d
計 a + c b + d a+b+c+d
検査異常の人
病気のある人
検査正常の人
病気のない人
感度100%、特異度100%なら完璧な検査
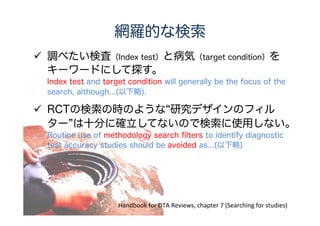
網羅的な検索の方法
調べたい検査(Index test)と病気(targetcondition)を
キーワードにして探す。
Index test and target condition will generally be the focus of the
search, although...(以下略).
RCTの検索の時のような“研究デザインのフィル
ター”は十分に確立してないので検索に使用しない。
Routine use of methodology search filters to identify diagnostic
test accuracy studies should be avoided as...(以下略)
Handbook for DTA Reviews, chapter 7 (Searching for studies)
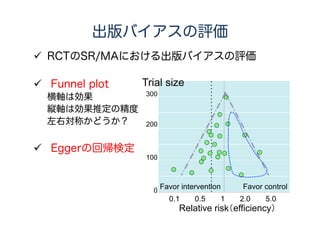
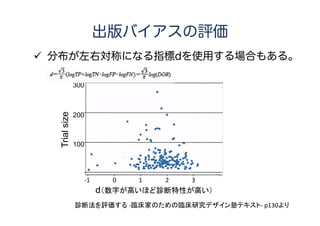
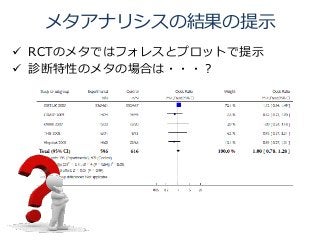
出版バイアスの評価
まだ評価方法が確立してないのでCochrane DTA
groupではオプション
Reviewauthors often elect not to investigate reporting bias
due to the lack of sensitive and appropriate statistical methods.
SR/MAは過去の研究だけどProtocolは多少大事
Similar arguments exist for systematic reviews,
but they are less strong because systematic reviews are
retrospective rather than prospective pieces of research.
参考:BMJグループの投稿規定
We strongly encourage you to register your study.
We recommend Prospero for registration of systematic reviews.
Handbook for DTA Reviews, chapter 4 (Guide to the contents of DTA protocol)
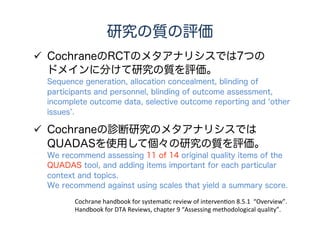
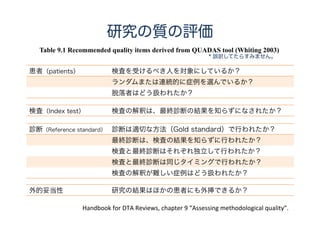
研究の質の評価
CochraneのRCTのメタアナリシスでは7つの
ドメインに分けて研究の質を評価。
Sequence generation,allocation concealment, blinding of
participants and personnel, blinding of outcome assessment,
incomplete outcome data, selective outcome reporting and ‘other
issues’.
Cochraneの診断研究のメタアナリシスでは
QUADASを使用して個々の研究の質を評価。
We recommend assessing 11 of 14 original quality items of the
QUADAS tool, and adding items important for each particular
context and topics.
We recommend against using scales that yield a summary score.
Cochrane handbook for systematic review of intervention 8.5.1 “Overview”.
Handbook for DTA Reviews, chapter 9 “Assessing methodological quality”.
24.
Handbook for DTAReviews, chapter 9 “Assessing methodological quality”.
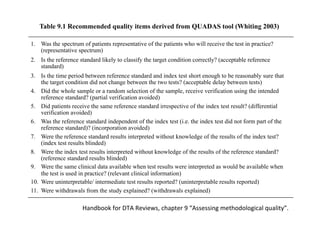
Table 9.1 Recommended quality items derived from QUADAS tool (Whiting 2003)
1. Was the spectrum of patients representative of the patients who will receive the test in practice?
(representative spectrum)
2. Is the reference standard likely to classify the target condition correctly? (acceptable reference
standard)
3. Is the time period between reference standard and index test short enough to be reasonably sure that
the target condition did not change between the two tests? (acceptable delay between tests)
4. Did the whole sample or a random selection of the sample, receive verification using the intended
reference standard? (partial verification avoided)
5. Did patients receive the same reference standard irrespective of the index test result? (differential
verification avoided)
6. Was the reference standard independent of the index test (i.e. the index test did not form part of the
reference standard)? (incorporation avoided)
7. Were the reference standard results interpreted without knowledge of the results of the index test?
(index test results blinded)
8. Were the index test results interpreted without knowledge of the results of the reference standard?
(reference standard results blinded)
9. Were the same clinical data available when test results were interpreted as would be available when
the test is used in practice? (relevant clinical information)
10. Were uninterpretable/ intermediate test results reported? (uninterpretable results reported)
11. Were withdrawals from the study explained? (withdrawals explained)
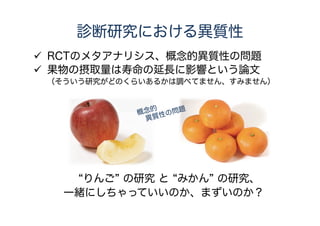
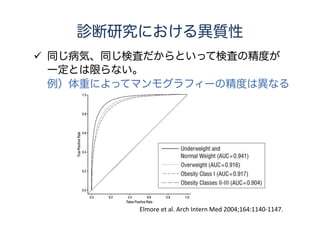
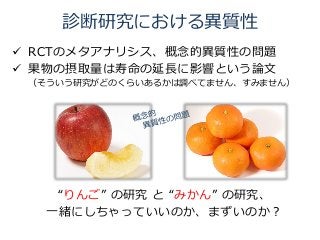
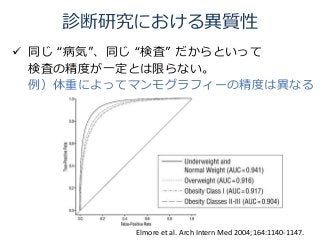
診断研究における異質性
同じ “病気”、同じ“検査” だからといって
検査の精度が一定とは限らない。
例)体重によってマンモグラフィーの精度は異なる
Elmore et al. Arch Intern Med 2004;164:1140-1147.
32.
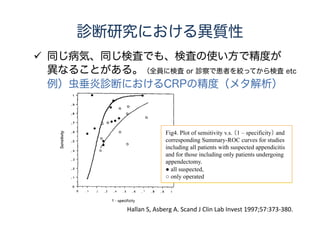
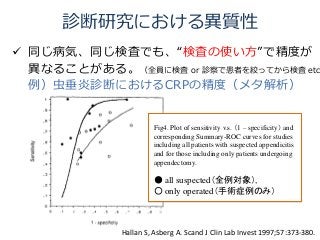
診断研究における異質性
同じ病気、同じ検査でも、“検査の使い方”で精度が
異なることがある。(全員に検査 or診察で患者を絞ってから検査 etc
例)虫垂炎診断におけるCRPの精度(メタ解析)
Hallan S, Asberg A. Scand J Clin Lab Invest 1997;57:373-380.
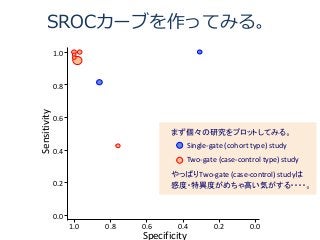
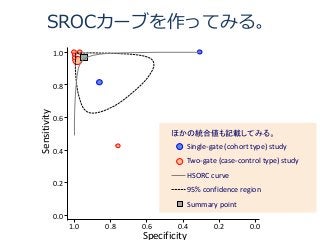
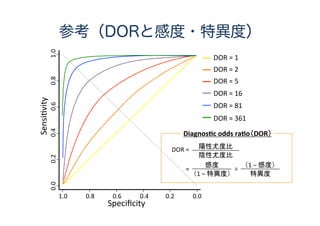
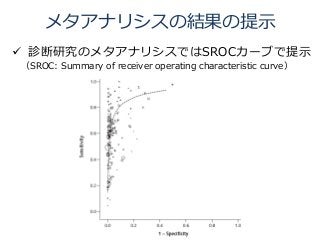
Fig4. Plot of sensitivity v.s. (1 – specificity) and
corresponding Summary-ROC curves for studies
including all patients with suspected appendicitis
and for those including only patients undergoing
appendectomy.
● all suspected(全例対象),
○ only operated(手術症例のみ)
SR/MAは事前登録すべきか?
前向き臨床試験におけるProtocolの事前登録
バイアスをなるべく避けるために大事
Pre-specificationof methods provides protection against some
aspects of bias and demonstrates scientific rigour.
SR/MAは過去の研究だけどProtocolは多少大事
Similar arguments exist for systematic reviews,
but they are less strong because systematic reviews are retrospecti
rather than prospective pieces of research.
参考:BMJグループの投稿規定
We strongly encourage you to register your study.
We recommend Prospero for registration of systematic reviews.
Handbook for DTA Reviews, chapter 4 (Guide to the contents of DTA protocol)
網羅的な検索のおさらい
調べたい検査(Index test)と病気(targetcondition)を
キーワードにして探す。
Index test and target condition will generally be the focus of the
search, although...(以下略).
RCTの検索の時のような“研究デザインのフィル
ター”は十分に確立してないので検索に使用しない。
Routine use of methodology search filters to identify diagnostic
test accuracy studies should be avoided as...(以下略)
Handbook for DTA Reviews, chapter 7 (Searching for studies)
48.
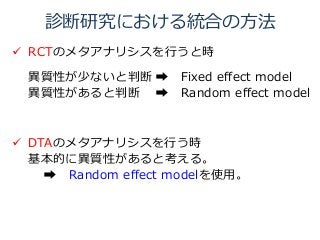
検索式を作ってみる。
#1 “epiglot* ”
#2“supraglot* ”
#3 ”laryngit* ”
#4 “laryngotracheit* ”
#5 “supraglottitis” [mesh]
#6 “laryngitis” [mesh]
#7 #1 OR #2 OR #3 OR #4 OR #5 OR #6
#8 “roentgen”
#9 “x-ray”
#10 “xp”
#11 “radiograph* ”
#12 “diagnostic imaging” [mesh]
#13 #8 OR #9 OR #10 OR #11 OR #12
#14 #7 and #13
キーワード検索
シソーラス検索
キーワード検索
シソーラス検索
調べたい病気
(Targetcondition)
調べたい検査
(Indextest)






![検索式を作ってみる。
#1 “epiglot* ”
#2 “supraglot* ”
#3 ”laryngit* ”
#4 “laryngotracheit* ”
#5 “supraglottitis” [mesh]
#6 “laryngitis” [mesh]
#7 #1 OR #2 OR #3 OR #4 OR #5 OR #6
#8 “roentgen”
#9 “x-ray”
#10 “xp”
#11 “radiograph* ”
#12 “diagnostic imaging” [mesh]
#13 #8 OR #9 OR #10 OR #11 OR #12
#14 #7 and #13
キーワード検索
シソーラス検索
キーワード検索
シソーラス検索
調べたい病気
(Targetcondition)
調べたい検査
(Indextest)](https://image.slidesharecdn.com/140709-140725204734-phpapp01/85/slide-48-320.jpg)