Downloaded 59 times













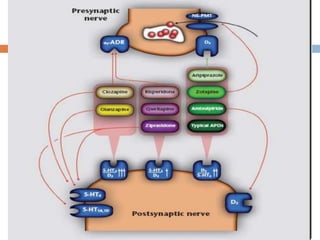




















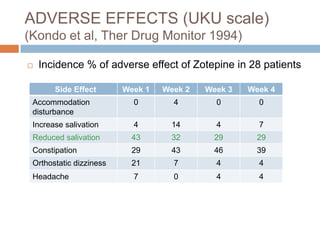






This document summarizes a presentation about the use of zotepine in psychiatric disorders. It discusses zotepine's classification as an atypical antipsychotic, its pharmacology and mechanisms of action, efficacy in treating schizophrenia and its symptoms, dosing, adverse effects, drug interactions, and use in special populations. Several studies are summarized that demonstrate zotepine's efficacy in acute exacerbation of schizophrenia, against hostility and negative symptoms, and for relapse prevention, with adverse effect profiles comparable or favorable to other antipsychotics.

















































































