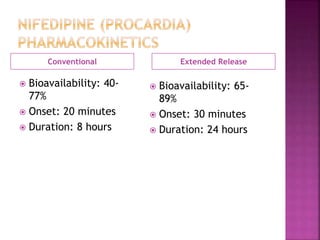
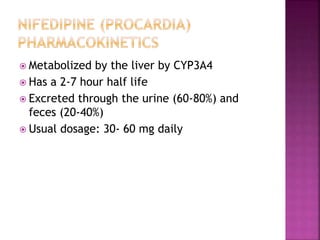
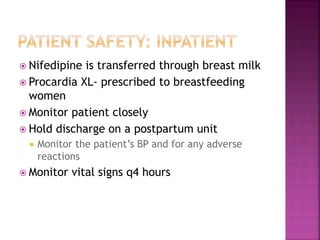
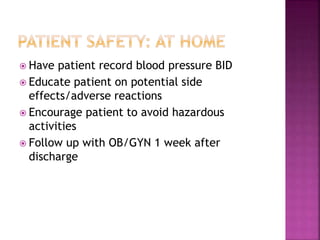
This document discusses preeclampsia and gestational hypertension, conditions that occur during pregnancy involving high blood pressure. It also discusses nifedipine (Procardia), a calcium channel blocker prescribed to treat hypertension during pregnancy and postpartum. The key effects of nifedipine are relaxing blood vessels to increase blood flow and reduce blood pressure. Common side effects and drug interactions are presented. Guidelines are provided for monitoring patients on nifedipine during the postpartum period.
![ Arcangelo, V. P., & Peterson, A. M. (2013).
Pharmacotherapeutics for advanced practice: A practical
approach (3rd ed.). Ambler, PA: Lippincott, Williams &
Cunha, J. (2015). Procardia. Retrieved from
http://www.rxlist.com/procardia-side-effects-drug-
center.htm
Koley, A. P., Robinson, R. C., Markowitz, A., & Friedman, F.
K. (1997). Drug-drug interactions: Effect of quinidine on
nifedipine binding to human cytochrome P450 3A4 [].
Biochemical Pharmacology, 54(4), 455-460. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/9105395
Murray, S. S., & McKinney, E. S. (2014). Foundations of
maternal-newborn and women’s health nursing (6th ed.).
St. Louis, MO:
Nifedipine (oral route). (2015). Retrieved from
http:www/mayoclinic.org/drugs-supplements/nifedipine-
oral-route/description/drg-20071680](https://image.slidesharecdn.com/nifedipineprocardia-151115144218-lva1-app6892/85/Nifedipine-procardia-13-320.jpg)