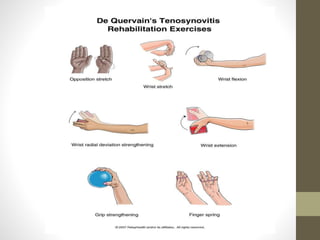
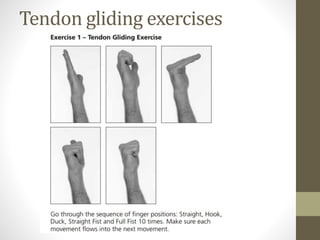
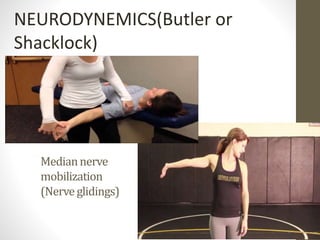
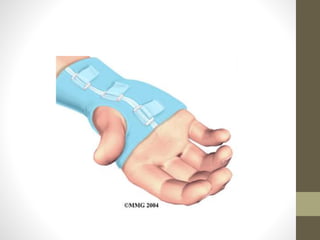
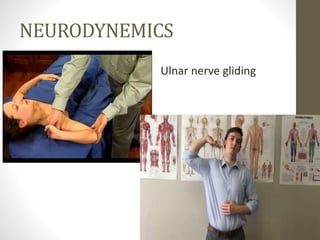
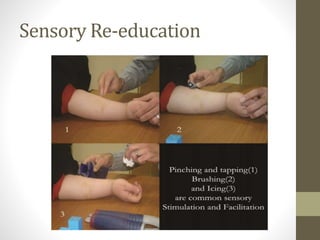
This document discusses the management of various wrist injuries including fractures, tendon injuries, nerve injuries, and joint injuries. For fractures, rehabilitation focuses on gradual mobilization and strengthening after immobilization. For tendon injuries like de Quervain's tenosynovitis, treatment involves splinting, stretching and strengthening exercises. Nerve injuries like carpal tunnel syndrome are initially treated with splinting and exercises before possible surgery. Rehabilitation for joint injuries like triangular fibrocartilage complex tears focuses on immobilization, bracing, strengthening and range of motion exercises. Modalities, nerve gliding exercises and sensory re-education are also used in managing various wrist conditions.