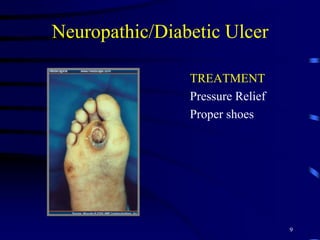
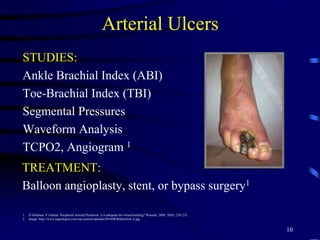
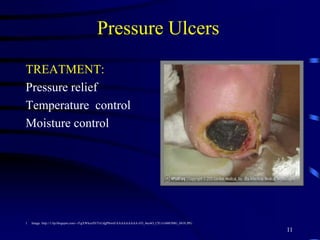
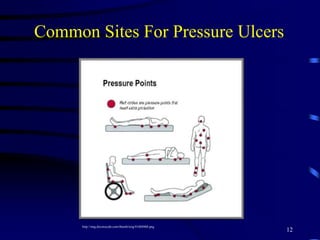
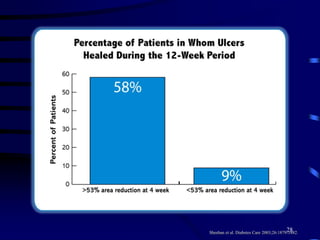
This document discusses wound care in the geriatric population. It outlines risk factors for wounds in older adults and describes assessing and managing different wound types like pressure ulcers, venous stasis ulcers, and diabetic foot ulcers. Standard wound treatments involve addressing underlying causes, cleaning the wound bed, and dressing changes. If wounds do not improve with standard care after 4 weeks, advanced therapies may be considered, such as skin substitutes, growth factors, and negative pressure wound therapy to aid healing. The goal is to diagnose and correct risk factors while managing the wound to assess progress and determine if specialized treatments could help non-healing or chronic wounds.





























































































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




