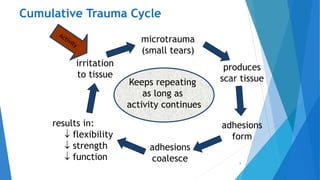
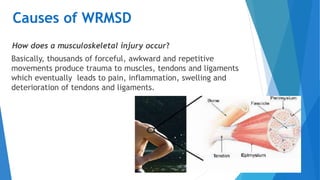
This document discusses work-related musculoskeletal disorders (WMSDs) of the elbow. It defines WMSDs as injuries or disorders of the muscles, tendons, and joints caused by repetitive strain from manual labor tasks. Common WMSDs of the elbow mentioned include lateral epicondylitis (tennis elbow), medial epicondylitis (golfer's elbow), cubital tunnel syndrome, bursitis, tendinitis of the distal bicep and triceps, and pronator teres syndrome. Risk factors include excessive force, awkward postures, repetition, direct pressure, vibration, and non-occupational factors like fitness level. Symptoms may include pain, numbness, swelling, and loss of flexibility