
Recommended
Recommended
More Related Content
Similar to Medial Epicondylitis conditioning and rehab
Similar to Medial Epicondylitis conditioning and rehab (20)
Recently uploaded
Recently uploaded (20)
Medial Epicondylitis conditioning and rehab
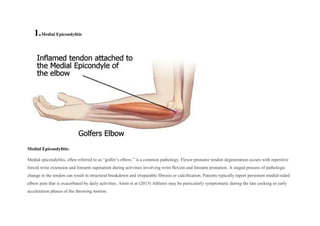
- 1. 1.Medial Epicondylitis Medial Epicondylitis: Medial epicondylitis, often referred to as “golfer’s elbow,” is a common pathology. Flexor-pronator tendon degeneration occurs with repetitive forced wrist extension and forearm supination during activities involving wrist flexion and forearm pronation. A staged process of pathologic change in the tendon can result in structural breakdown and irreparable fibrosis or calcification. Patients typically report persistent medial-sided elbow pain that is exacerbated by daily activities. Amin et at (2015) Athletes may be particularly symptomatic during the late cocking or early acceleration phases of the throwing motion.
- 2. The part of the muscle that attaches to a bone is called a tendon. Some of the muscles in your forearm attach to the bone on the inside of your elbow. When you use these muscles over and over again, small tears may develop in the tendons. Over time, this leads to irritation and pain where the tendon is attached to the bone.
- 3. The injury can occur from using poor form or overdoing certain sports, such as: Golf Baseball and other throwing sports, such as American football and javelin Baseball
- 4. American football Javelin Racquet sports: Improper technique with tennis strokes, especially the backhand, can cause injury to the tendon. Excessive use of topspin and using a racket that's too small or heavy also can lead to injury.
- 5. Tennis Weight training: Lifting weights using improper technique, such as curling the wrists during a biceps exercise, can overload the elbow muscles and tendons.
- 7. Repeated twisting of the wrist (such as when using a screwdriver) can lead to golfer's elbow. People in certain jobs may be more likely to develop it, such as: Painters Plumbers Construction workers Cooks Assembly-line workers Computer users Butchers Anatomy:
- 8. The flexor-pronator tendon is the confluence of five muscles of the forearm: the pronator teres (PT), flexor carpi radialis, palmaris longus, flexor carpi ulnaris (FCU), and flexor digitorum superficialis (Figure B). This CFT is approximately 3 cm long and, in most elbows, crosses the ulnohumeral joint medially. The tendon attaches to the medial humeral epicondyle anteriorly and attaches proximally to the anterior bundle of the ulnar collateral ligament (UCL), with the fibers parallel to the UCL. Otoshi, K.,(2014). The CFT, particularly the ulnar head of the PT, also becomes confluent with a hyperplastic section of the anteromedial joint capsule.
- 9. Most authors believe the principle mechanism of injury is repetitive eccentric loading of the muscles conducting wrist flexion and forearm pronation combined with valgus overload at the elbow. Barco, R et al (2017). Strain of the medial elbow with a valgus overload moment, which occurs with overhead throwing, stimulates dynamic stabilization of the joint via eccentric contraction of the CFT. Lynch JR. et al (2008) simultaneous wrist flexion or forearm pronation during ball release may produce even greater eccentric stress on the tendon. Sisto DJ et al (1982) Historically, the Pronator Teres has been identified as the primary dynamic stabilizer and the most likely musculotendinous unit to be injured in medial epicondylitis. Recent cadaver studies, however, have implicated every musculotendinous unit except the palmaris longus. Repetitive supraphysiologic stress on the tendon eventually results in microtrauma and degeneration. Histopathologic examination has revealed a staged process of pathologic tendon change. Riley, G. (2004) Initially, repetitive trauma results in peritendinous inflammation. Continued injury results in angiofibroblastic hyperplasia, an invasion of vascular and fibroblastic elements into the tendon. Eventually, replacement of the normal tendon with angiofibroblastic hyperplasia results in structural breakdown and irreparable fibrosis or calcification. Activity causing such pathology to the CFT can eventually transfer forces deeper to the UCL, which mirrors CFT fiber orientation and histologic anatomy. Risk Factors: Medial epicondylitis, or “golfer’s elbow,” is a pathology commonly encountered by orthopaedic surgeons. Despite an overall prevalence of <1%, medial epicondylitis may affect as many as 3.8% to 8.2% of patients in occupational settings. Raham et al (2006) Medial-sided pathology can be found in as many as 10% to 20% of patients with epicondylitis. Baumgard et al (1982) A result of common flexor tendon (CFT) microtrauma and degeneration, medial epicondylitis typically occurs in the fourth through sixth decades of life, Descatha et al (2003) the peak working years noted nearly a 2:1 ratio of occurrence for women compared to men with a diagnosis of medial epicondylitis. Shiri et al (2006) Overuse: Repetitive wrist and forearm movements, such as gripping, twisting, and lifting, can lead to the condition. Descatha, A et al (2013).
- 10. Age: It is more common in individuals between 40 and 60 years old. Seems to effect women is more then men. Shiri, R. et al, (2011) Work and Hobbies: Occupations or activities that involve repetitive arm and wrist motions. Biomechanical Factors: Poor technique or equipment in sports and activities. Ciccotti, M. G., & Ramani, M. N. (2003). Muscle Imbalances: Weak forearm muscles can contribute to the development of medial epicondylitis. Signs and Symptoms: Symptoms of golfer's elbow include:
- 11. golfer's elbow are associated with decreased normalized eccentric peak torque ( NEPT) of shoulder external rotators and abductors compared with those of healthy athletes. This tends to decrease the external stability of the shoulder joint and put high stress on the distal joints of the upper kinetic chain. Nabil BA, et al ( 2019) Elbow pain that runs along the inside of your forearm to your wrist, on the same side as your pinky finger Pain when flexing your wrist, palm down Pain when shaking hands Weak grasp Numbness and tingling from your elbow up and into your pinky and ring fingers (due to irritation of the ulnar nerve in this region) Pain may occur gradually or suddenly. It gets worse when you grasp things or flex your wrist. Aggravating Factors: Overhead throwing athletes and those participating in sports that require repeated forearm pronation and wrist flexion are most commonly affected by this disorder. Mishra,et al (2014). It seems to be more common among athletes, including golfers (the source of “golfer’s elbow”), throwing athletes, baseball players and tennis players Descatha A. et al (2003) Forceful Gripping: Activities that require a strong grip, like using hand tools, racquet sports, or heavy lifting.
- 12. Incorrect Technique: Poor sports or work technique can contribute to the development or exacerbation of medial epicondylitis. Prevention You can take steps to prevent golfer's elbow: Strengthen your forearm muscles. Use light weights or squeeze a tennis ball. Even simple exercises can help your muscles absorb the energy of sudden physical stress. Stretch before your activity. Walk or jog for a few minutes to warm up your muscles. Then do gentle stretches before you begin your game. Fix your form. Whatever your sport, ask an instructor to check your form to avoid overload on muscles. Use the right equipment. If you're using older golfing irons, consider upgrading to lighter graphite clubs. If you play tennis, make sure your racket fits you. A racket with a small grip or a heavy head may increase the risk of elbow problems. Lift properly. When lifting anything — including free weights — keep your wrist rigid and stable to reduce the force to your elbow. Know when to rest. Try not to overuse your elbow. At the first sign of elbow pain, take a break. Rehabilitation Exercises (Different Stages):
- 13. Phase 1 (Pain Control): Rest, ice, and anti-inflammatory medications to reduce pain and inflammation. Gentle range of motion exercises, isometrics, and wrist and forearm stretches. Phase 2 (Strengthening): Gradual introduction of resistance exercises targeting the forearm and wrist. Eccentric exercises for the wrist flexors and concentric exercises to build strength. Phase 3 (Functional): Incorporate functional movements that mimic daily activities or sport-specific motions. For example, golf swings, bat swings, or tool use, based on individual needs and goals. Pathology:Medial Epicondylitis PHASE: Early (rough time frame - ………………………0-4 weeks………) Goals 1.Reduce pain and inflamation 2. improve flexibility and range of motion Exercise Rationale (Aim/ component of fitness/tissue type) Reps/ Time Sets Rest Other… Tempo/Inten 1. Wrist stretches Stretching to alleviate tension in the affected muscles 30 sec hold 10 reps 3 30 sec Perform after activity or when feeling tiredness
- 14. 2. Towel Grip Strength Place a Rolled up towel in your hand and squeeze 15 reps/ hold 2 sec 3 30 sec Slow and controlled movement , focus on the lowering phase
- 15. 3.Resisted elbow flexion and extension Strengthening the forearm muscles to support the elbow joint 12 reps 3 30 sec Use light resistance initially, gradually increase as tolerated PHASE: Intermediate (rough time frame - ………4-8 weeks………………………) Goals 1.increase strength and endurance of the forearm muscles 2.improve stability of the elbow joint Exercise Rationale (Aim/ component of fitness/tissue type) Reps/ Time Sets Rest Other… Tempo/Inten 1.Eccentric wrist flexion Strengthening the wrist flexors eccentrically to promote tendon healing and strength 10 reps 3 30 sec Slow and controlled movement , focus on the
- 16. lowering phase 2.Theraband flexion/ extension Resistance training to further strengthen the wrist flexors and extensors 15 reps 3 30 sec Use a theraband or resistance tubing, increase resistance gradually 3.Eccentric pronation/supination Strengthinig eccentrically to improve tendon resilience and strength 10 reps 3 30 sec Focus on controlled movement during the lowering phase
- 17. PHASE: Late (rough time frame - ………8-12 weeks………………………) Goals 1. Full restoration of strength and function 2. prevention of recurrence Exercise Rationale (Aim/ component of fitness/tissue type) Reps/ Time Sets Rest Other… Tempo/Inten 1. Shoulder external rotation with cable pulley 90-90 This exercise targets the rotator cuff muscles, specifically the external rotators, to improve shoulder stability and prevent compensatory movements. 8 3 60sec Perform the movement with controlled and deliberate motion, focusing on maintaining proper form
- 18. throughout the range of motion. 2. Shoulder Lateral raises with dumbles (scaption raise) This exercise targets the deltoid muscles, particularly the middle deltoid, to improve shoulder strength and stability. 10 3 45 sec Perform the movement with a controlled and smooth motion, avoiding swinging or momentum. Focus on lifting the dumbbells to shoulder height in line with the shoulders and maintaining a slight bend in the elbows. 3. Shoulder pull overs with cable This exercise targets the muscles of the shoulder girdle and upper back, including the lats and serratus anterior, to improve shoulder stability and strength. 10 3 60sec Perform the movement with controlled
- 19. resistance, focusing on engaging the muscles of the shoulder and upper back throughout the exercise. Maintain a stable core and avoid overarching the lower back. References: Amin, N. H., Kumar, N. S., & Schickendantz, M. S. (2015). Medial epicondylitis: evaluation and management. JAAOS-Journal of the American Academy of Orthopaedic Surgeons, 23(6), 348-355. Barco, R., & Antuña, S. A. (2017). Medial elbow pain. EFORT Open Reviews, 2(8), 362-371. Retrieved Feb 6, 2024, from https://doi.org/10.1302/2058-5241.2.160006 Baumgard SH, Schwartz DR. Percutaneous release of the epicondylar muscles for humeral epicondylitis. The American Journal of Sports Medicine. 1982;10(4):233-236. doi:10.1177/036354658201000408
- 20. Bisset L, Beller E, Jull G, Brooks P, Darnell R, Vicenzino B. "Mobilization with movement and exercise, corticosteroid injection, or wait and see for golfers elbow: randomised trial." British Medical Journal. 2006;333(7575):939. Ciccotti, M. G., & Ramani, M. N. (2003). Medial epicondylitis. Techniques in hand & upper extremity surgery, 7(4), 190-196. Descatha A , Leclerc A , Chastang JF , Roquelaure Y : Medial epicondylitis in occupational settings: prevalence, incidence and associated risk factors . J Occup Environ Med 2003 ; 45: 993 – 1001 . Descatha A, Leclerc A, Chastang JF, Roquelaure Y; Study Group on Repetitive Work. Medial epicondylitis in occupational settings: prevalence, incidence and associated risk factors. J Occup Environ Med. 2003 Sep;45(9):993-1001. doi: 10.1097/01.jom.0000085888.37273.d9. PMID: 14506342; PMCID: PMC4850209. Descatha, A., Dale, A. M., Jaegers, L., Herquelot, E., & Evanoff, B. (2013). Self-reported physical exposure association with medial and lateral epicondylitis incidence in a large longitudinal study. Occupational and environmental medicine. Lynch JR, Waitayawinyu T, Hanel DP, Trumble TE. Medial collateral ligament injury in the overhand-throwing athlete. J Hand Surg Am. 2008 Mar;33(3):430-7. doi: 10.1016/j.jhsa.2007.12.015. PMID: 18343303. Mishra, Allan MD*; Pirolo, Joseph M. MD†; Gosens, Taco MD, PhD‡. Treatment of Medial Epicondylar Tendinopathy in Athletes. Sports Medicine and Arthroscopy Review 22(3):p 164-168, September 2014. | DOI: 10.1097/JSA.0000000000000031 Nabil BA, Ameer MA, Abdelmohsen AM, Hanafy AF, Yamani AS, Elhafez NM, Elhafez SM. The Impact of Tennis and Golfer's Elbow on Shoulder External Rotators and Abductors' Peak Torque. J Sport Rehabil. 2019 Nov 26;29(4):469-475. doi: 10.1123/jsr.2018-0159. PMID: 31034312. Otoshi, K., Kikuchi, Si., Shishido, H. et al. The proximal origins of the flexor–pronator muscles and their role in the dynamic stabilization of the elbow joint: an anatomical study. Surg Radiol Anat 36, 289–294 (2014). https://doi.org/10.1007/s00276-013-1168-3
- 21. Paoloni JA, Murrell GA, Burch R, et al. "Randomised, double-blind, placebo-controlled clinical trial of a new topical glyceryl trinitrate patch for chronic medial epicondylitis." British Journal of Sports Medicine. 2009;43(4):299-302. Rahman Shiri, Eira Viikari-Juntura, Helena Varonen, Markku Heliövaara, Prevalence and Determinants of Lateral and Medial Epicondylitis: A Population Study, American Journal of Epidemiology, Volume 164, Issue 11, 1 December 2006, Pages 1065– 1074, https://doi.org/10.1093/aje/kwj325 Riley, G. (2004). Tendon and ligament biochemistry and pathology. Soft tissue rheumatology, 2053, 3-39. Shiri R , Viikari-Juntura E , Varonen H , Heliovaara M : Prevalence and determinants of lateral and medial epicondylitis: a population study . Am J Epidemiol 2006 ; 164: 1065 – 74 . Shiri, R., & Viikari-Juntura, E. (2011). Lateral and medial epicondylitis: role of occupational factors. Best practice & research Clinical rheumatology, 25(1), 43-57. Sisto DJ, Jobe FW, Moynes DR, Antonelli DJ. An electromyographic analysis of the elbow in pitching. The American Journal of Sports Medicine. 1987;15(3):260-263. doi:10.1177/036354658701500314 Walker-Bone K , Palmer KT , Reading I , Coggon D , Cooper C : Prevalence and impact of musculoskeletal disorders of the upper limb in the general population . Arthritis Rheum 2004 ; 51: 642 – 51 .