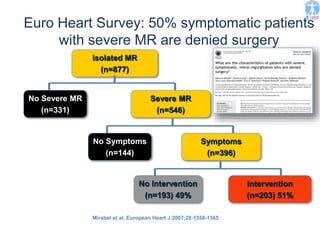
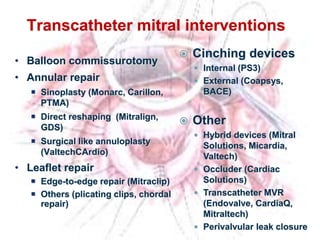
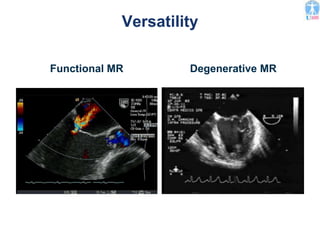
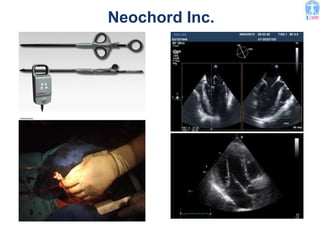
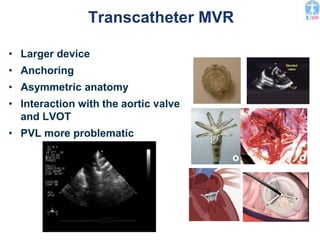
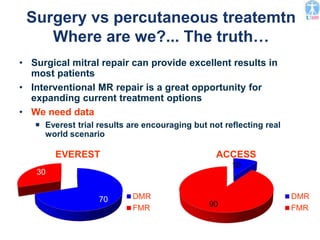
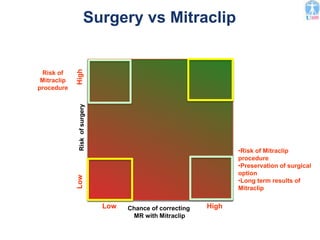
This document summarizes the current status of surgical and transcatheter mitral valve repair. It notes that mitral valve repair surgery has low risks and good outcomes when appropriate procedures are used. However, around 50% of symptomatic patients with severe mitral regurgitation are denied surgery. New transcatheter techniques are being developed as alternatives to surgery, including the MitraClip edge-to-edge repair device, annuloplasty devices, and future prospects for transcatheter mitral valve replacement. Early experiences with MitraClip show it reduces mitral regurgitation in many patients but long-term outcomes need further study. An individualized approach is needed to determine the best repair option based on a patient's anatomy,


































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)












