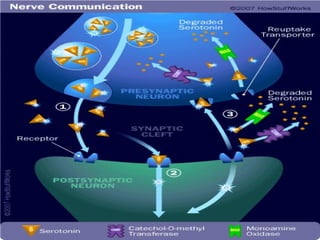
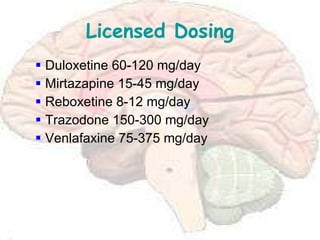
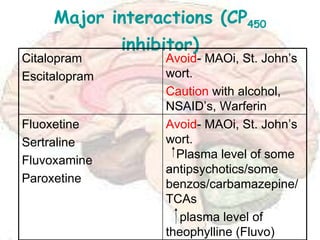
SSRIs and SNRIs are commonly used to treat depression. SSRIs work by blocking the reuptake of serotonin, increasing levels of the neurotransmitter in the brain. Common SSRIs include fluoxetine, paroxetine, sertraline, and citalopram. SNRIs like venlafaxine also block the reuptake of serotonin and norepinephrine. These drugs are generally well-tolerated but side effects may include nausea, insomnia, sexual dysfunction, and agitation. Guidelines recommend SSRIs as first-line treatment for moderate to severe depression.