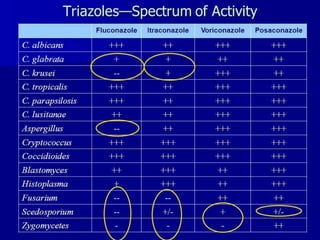
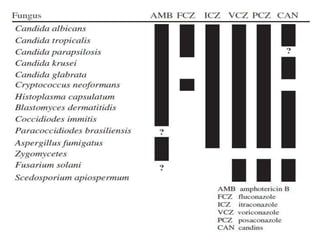
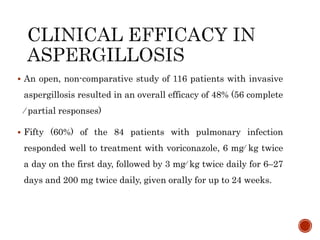
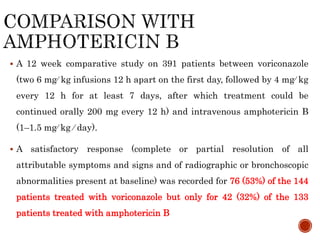
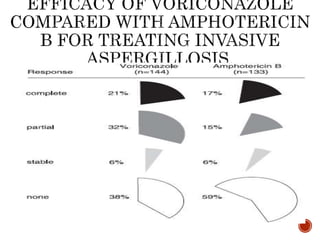
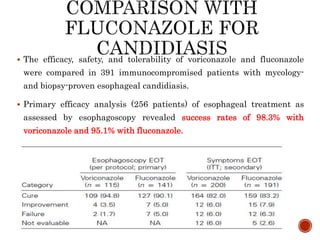
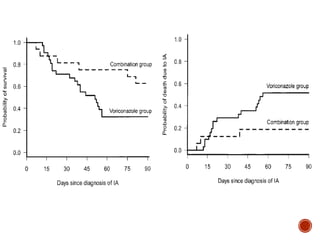
Fungal infections remain a major cause of illness and death, especially in immunocompromised patients. Voriconazole is a broad-spectrum triazole antifungal that is effective against a wide range of fungi including Aspergillus and Candida. Studies have shown voriconazole to have higher response and survival rates compared to amphotericin B for invasive aspergillosis. It is also as effective as fluconazole for esophageal candidiasis. Voriconazole can be used alone or in combination with other antifungals as salvage therapy for refractory infections.






























































![Continuous rrt and its role in critically ill patients [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/continuousrrtanditsroleincriticallyillpatientsautosaved-180707065857-thumbnail.jpg?width=640&height=640&fit=bounds)









![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













