Downloaded 88 times


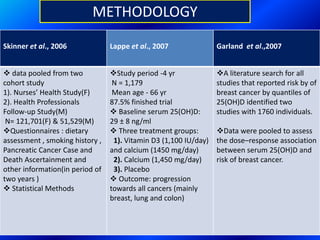
![TERMINOLOGY
• Cholecalciferol is the naturally occurring form of vitamin D.
Cholecalciferol is made in large quantities in skin when its exposed to
sunlight (UV – B rays 290 to 310 nm)
• Calcidiol’s main importance is that it is the storage form of vitamin D.
Serum 25-hydroxyvitamin D [25(OH)D] is the most reliable indicator of
vitamin D adequacy of an individual and also depicts the status of
vitamin D stores of an individual.
• Calcitriol (1,25- dihydroxy-vitamin D) is made from calcidiol in both the
kidneys and in other tissues and is the most potent steroid hormone
derived from cholecalciferol.
5](https://image.slidesharecdn.com/vitd-151125051726-lva1-app6892/85/VITAMIN-D-5-320.jpg)

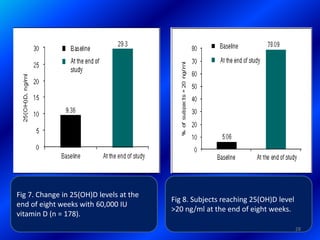
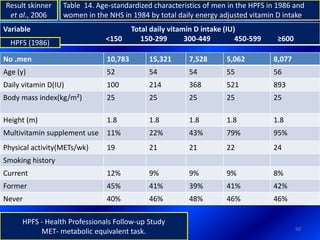
![29
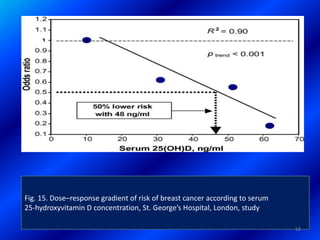
Result : Kumar et al., 2014
Body mass index were lower (adjusted P = 0.003) in the vitamin D Group
[1.18 (SD 0.92)] when compared with the placebo [1.02 (SD 0.91)] group
as a result of slightly lower weight and greater height.
The vitamin D group also had lower thigh circumference, arm muscle
area and slightly lower midupper arm circumference.
There were no group differences in body fat percentage, bone QUS or
blood pressure and few differences in motor development measures.
Vitamin D supplementation to lowbirth weight infants in infancy resulted
in children being thinner at age 36 years but no differences in functional
outcomes.](https://image.slidesharecdn.com/vitd-151125051726-lva1-app6892/85/VITAMIN-D-29-320.jpg)


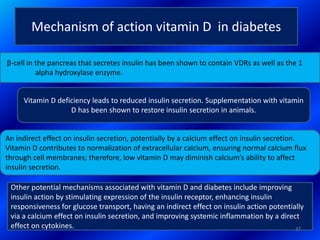
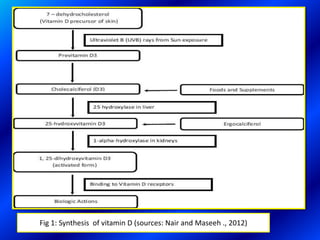
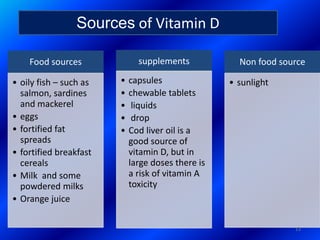
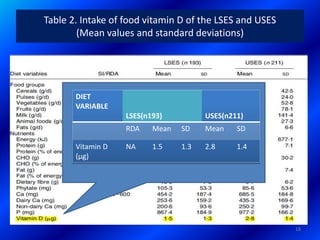
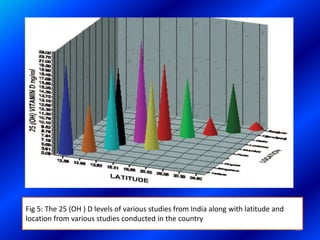
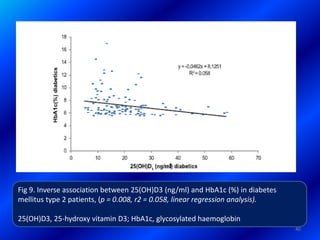
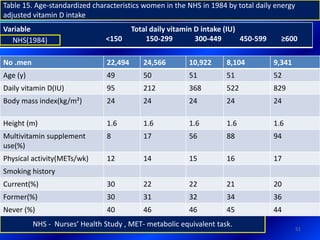
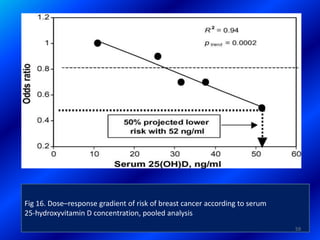
![Table 10 . 25(OH)D3 (ng/ml) (mean ± SEM), HbA1c (%) (mean ±
SEM) in the diabetes mellitus type 2 patients and controls and
statistical significance (Student’s t-test)
Subjects HbA1c (%) mean ±
SEM
25(OH)D3 (ng/ml) mean
± SEM
25(OH)D3
≤ 10 ng/ml < 20 ng/ml
Patients (n = 120)
7.2±0.18 19.26±0.94 21 (17.5%) 76 (63.3%)
Controls (n = 120)
5.1±0.05 25.48±1.02 7 (5.8%) 28 (23.3%)
Statistical
significance p < 0.001 p < 0.001 p = 0.0089 p < 0.0001
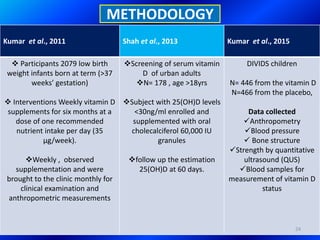
Results of
Athanassiou et
al ., 2013
number and percentage of subjects with 25(OH)D3 deficiency and insufficiency [25(OH)D3
≤ 10 ng/ml and < 20 ng/ml] in the patient and control groups and statistical significance
(chi-squared test).
39](https://image.slidesharecdn.com/vitd-151125051726-lva1-app6892/85/VITAMIN-D-39-320.jpg)

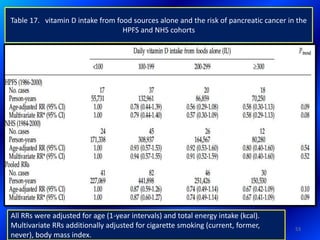



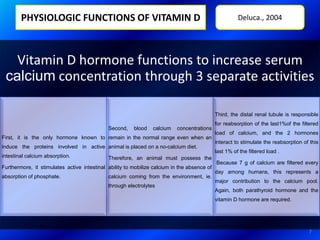
The seminar presents an extensive overview of vitamin D, highlighting its unique dual role as both a vitamin and hormone, essential for calcium homeostasis and various non-skeletal diseases. Recent studies indicate vitamin D's involvement in hormonal regulation, immune function, and cellular differentiation, linking deficiencies to several health conditions in the Indian population. It emphasizes the importance of adequate vitamin D levels obtained through sunlight exposure and dietary sources to mitigate risks of diseases like diabetes, cancer, and cardiovascular issues.








































![VITAMIN D[ SUNSHINE VITAMIN] MEDICINAL CHEMISTRY BY P. RAVISANKAR, CHEMISTRY ...](https://cdn.slidesharecdn.com/ss_thumbnails/02fat-solublevitamins-130615192714-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)














































