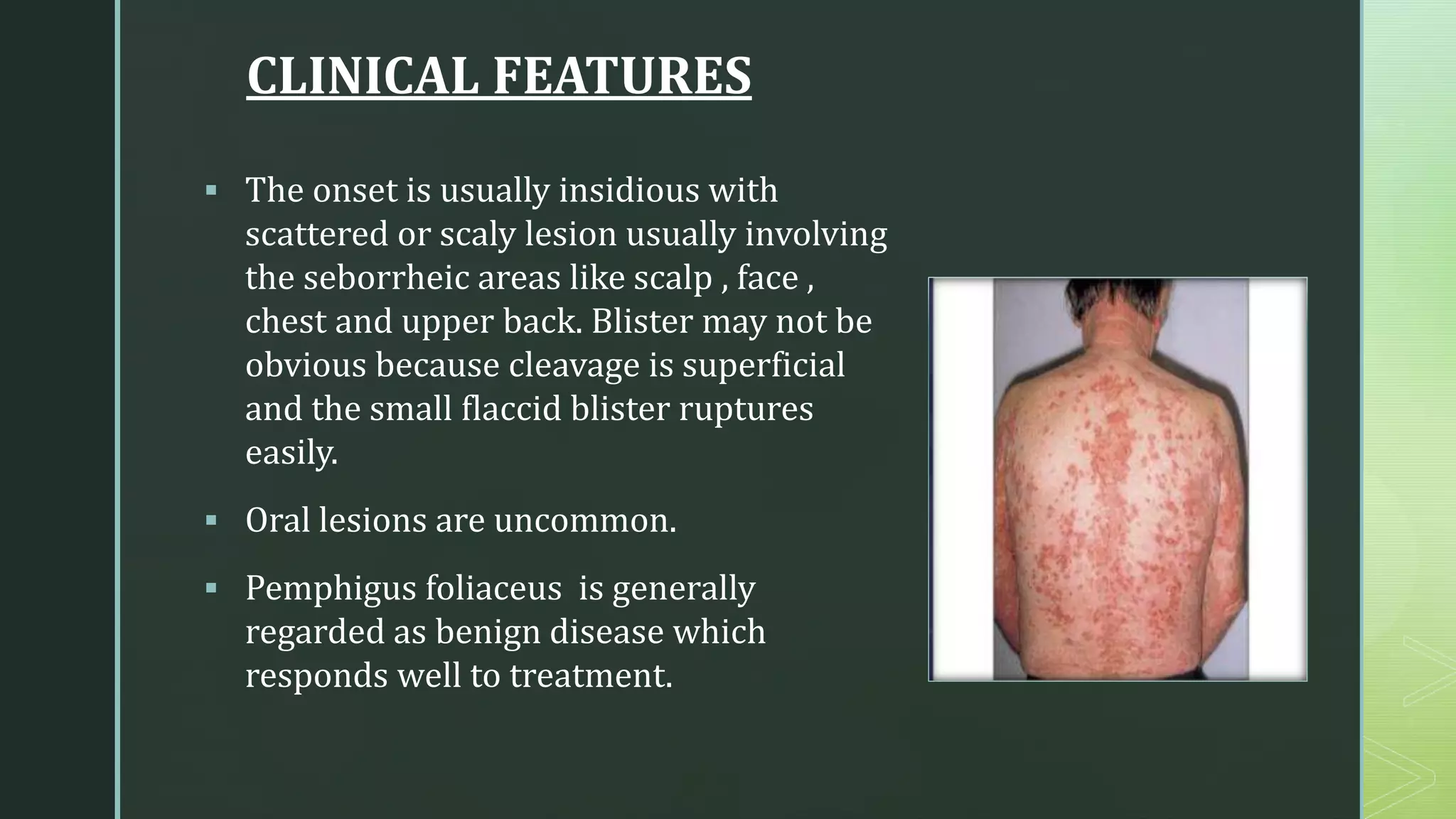
The document discusses various vesiculobullous lesions such as pemphigus vulgaris, pemphigus foliaceus, and bullous pemphigoid, detailing their clinical features, diagnosis, and management strategies. Pemphigus vulgaris is an autoimmune disease that can be fatal if untreated, while pemphigus foliaceus is considered benign and responds well to treatment. Erythema multiforme, characterized by abrupt onset and a variety of presentations, is also addressed, alongside supportive management options.


























































![[Chronic Multiple ulcers] O.Medicine lab](https://cdn.slidesharecdn.com/ss_thumbnails/o-250128123323-29e53ff5-thumbnail.jpg?width=640&height=640&fit=bounds)










































