Downloaded 41 times
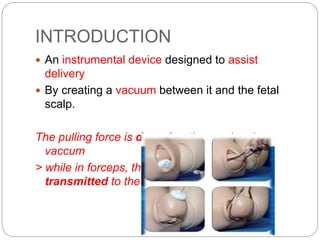
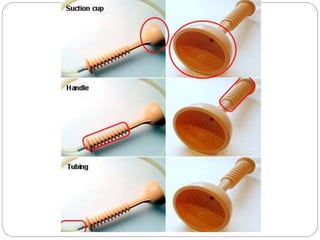
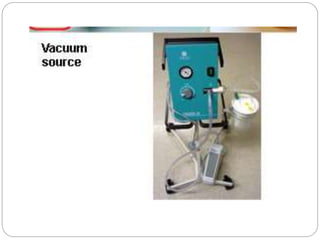








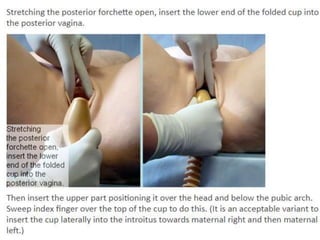


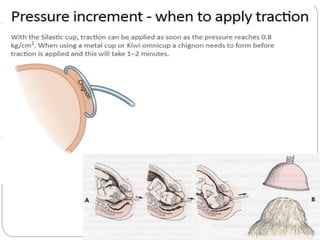
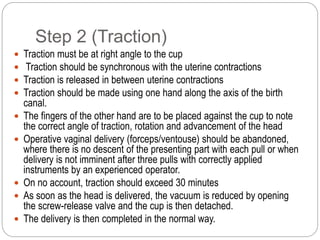
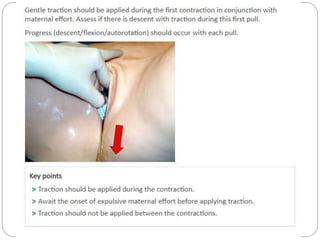
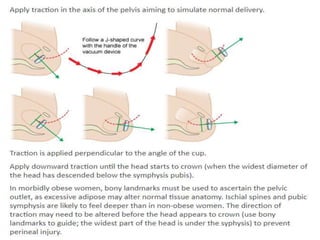
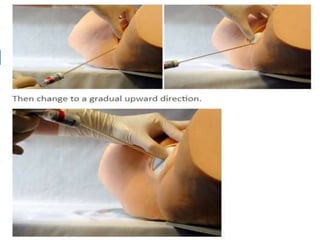
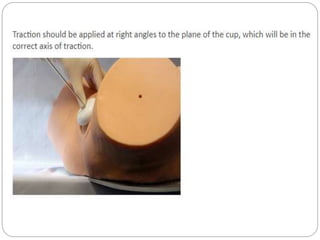

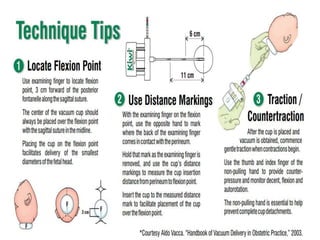
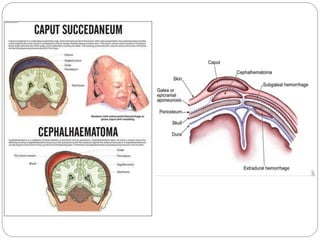


The document discusses the ventouse, an instrument used to assist childbirth by creating a vacuum between a suction cup and the fetal scalp. It describes the parts of the ventouse including soft silicone cups connected by tubing to a hand or electric pump. The document outlines the indications, contraindications, procedures and complications of ventouse delivery. Procedures include applying the cup to the fetal head and creating vacuum before gently tractioning the head during contractions. Potential neonatal complications include scalp abrasions while maternal complications are rare if soft tissues are not entrapped in the cup.























































































