Downloaded 14 times
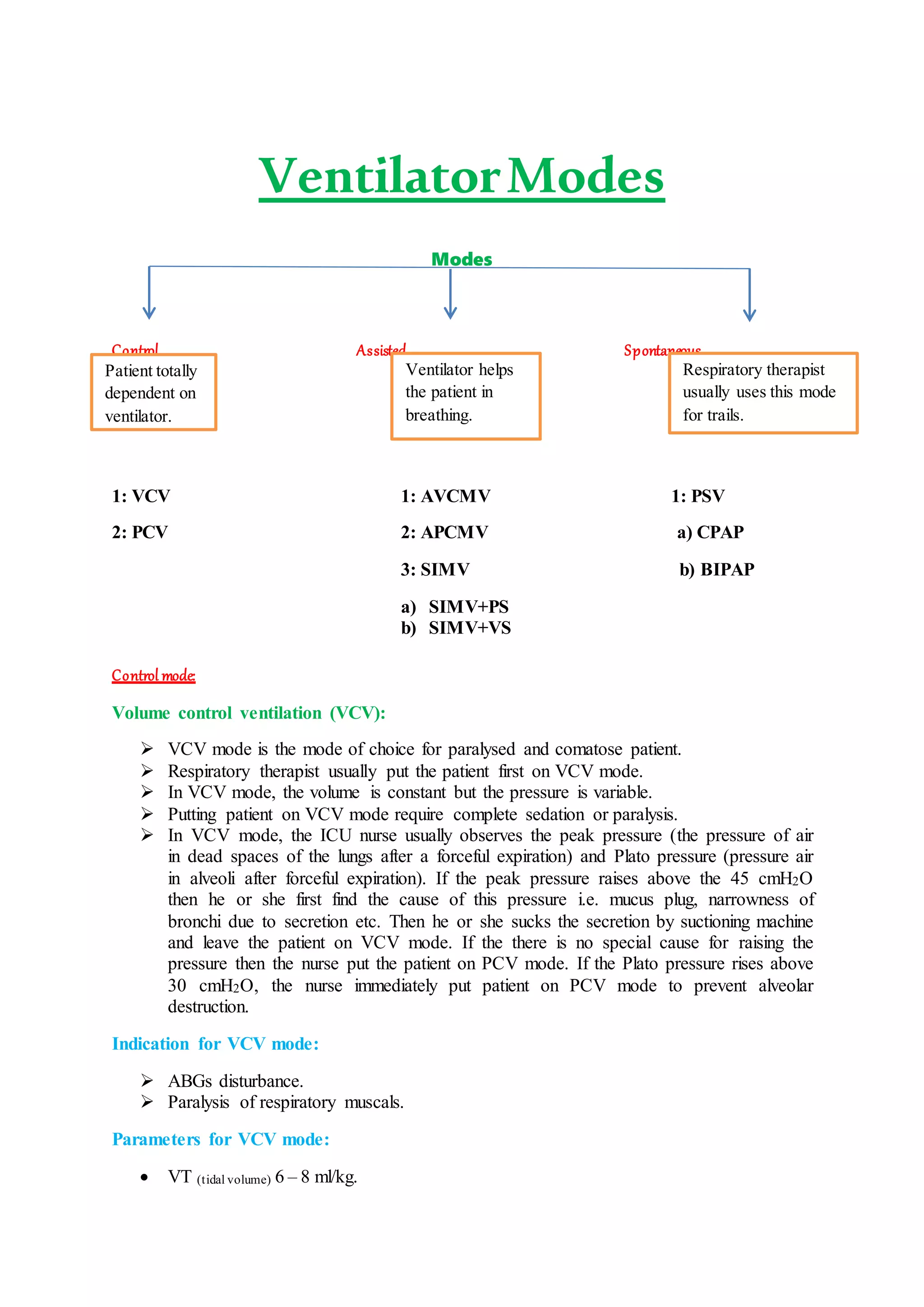




There are three main categories of ventilator modes: control, assisted, and spontaneous. Control modes like volume control ventilation (VCV) are used for paralyzed or comatose patients where the ventilator controls breathing. Assisted modes like assisted volume control mandatory ventilation (AVCMV) help patients breathe by providing a minimum tidal volume. Spontaneous modes like positive airway pressure (CPAP/BIPAP) allow breathing without machine triggers and are used non-invasively. Each mode has parameters that can be adjusted based on patient needs like tidal volume, respiratory rate, pressures, and more to provide appropriate ventilation support.



































































