Downloaded 19 times

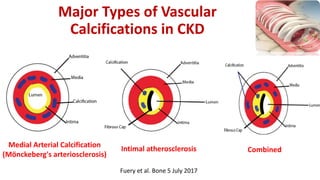
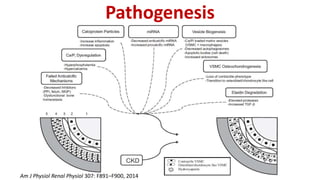

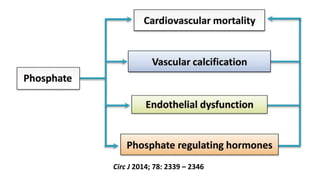
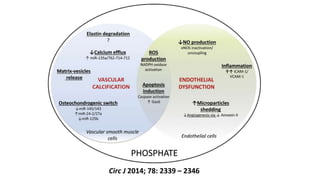
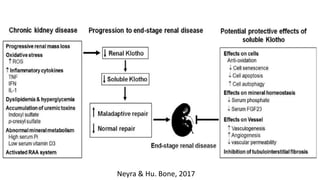
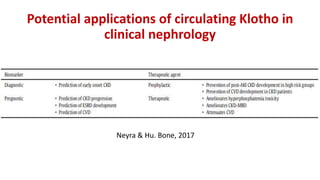
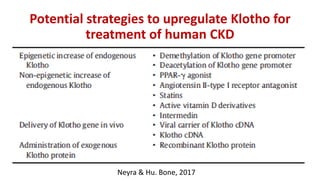
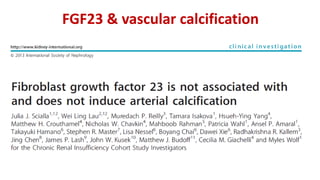
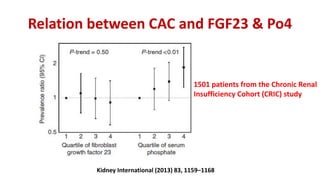
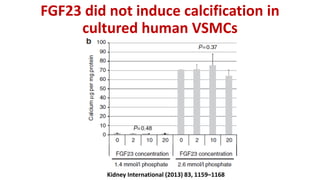
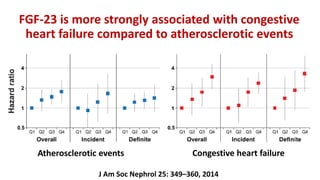
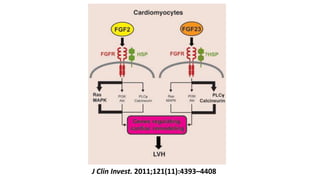
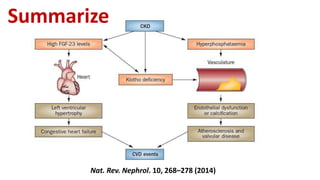






This document summarizes vascular calcification in patients with chronic kidney disease. It discusses several key factors involved in the pathogenesis of vascular calcification: 1) Phosphorus and fibroblast growth factor 23 (FGF23) levels are strongly associated with cardiovascular morbidity and mortality. High phosphorus and FGF23 levels may directly promote vascular calcification. 2) Klotho, the co-receptor for FGF23, plays an important role in phosphorus homeostasis and its downregulation is linked to vascular calcification. 3) Other factors discussed include vitamin D, alkaline phosphatase, magnesium, vitamin K, sclerostin, and other proteins that may influence vascular calcification. Understanding the complex interplay between these various



















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



