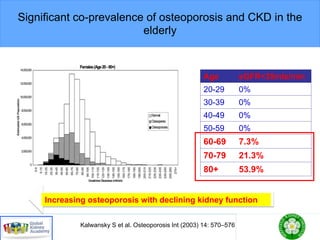
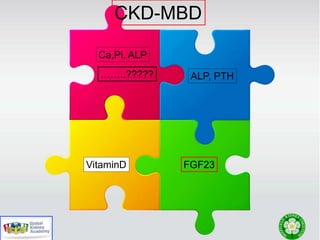
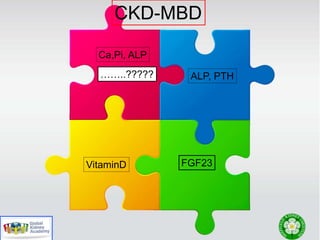
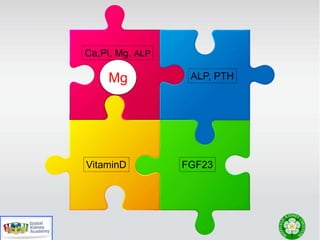
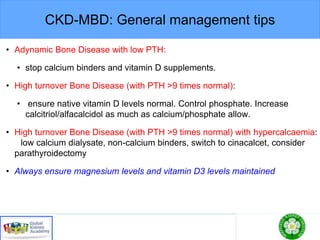
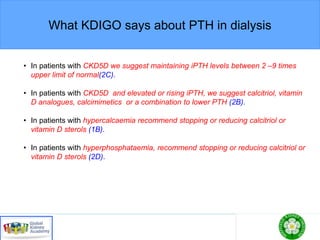
This document discusses chronic kidney disease-mineral and bone disorder (CKD-MBD). It begins with an overview of the key components involved in CKD-MBD, including calcium, phosphorus, parathyroid hormone, vitamin D, fibroblast growth factor 23, and magnesium. The document then presents two clinical cases involving patients with CKD and discusses treatment options based on their lab results. It also covers the roles of vitamin D and magnesium in vascular pathology and mortality in CKD patients. Guidelines for the treatment of secondary hyperparathyroidism from KDIGO are also summarized.








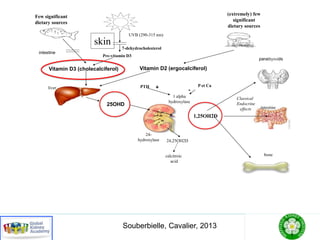
![Native Vitamin D Epidemiology
Definition
• Insufficiency: [25(OH)D] < 30 ng/mL
• Deficiency: [25(OH)D] < 10-15 ng/mL
Causes
• CKD is associated with 25OH VitaminD deficiencies
Prevalence
• Differences with age, ethnicity, latitude, culture and seasons
• In US HD Patients:
• Insufficiency: 78%, Deficiency: 18%](https://image.slidesharecdn.com/ckdmbdgcc2017final2-190412163306/85/CKD-MBD-2017-34-320.jpg)






![FGF23 and CKD
lotho levelsof CKD patients have been
ein thevery early stagesof CKD and to
KD progresses [36]. In a rodent CKD
vels in plasma, urine, and kidney were
se in parallel [36], but the relationship
elsin CKD patientsremainsto bedeter-
ore, almost all modelsof CKD, includ-
avebeen createdbyrenal tissueablation,
tis, nephrotoxin, diabetic nephropathy,
e kidney damage, are characterized by
wnregulation of Klotho mRNA and pro-
ey and by low plasma or urine-soluble
]. Plasma soluble Klotho levels are also
early stagesof CKD [58].Pavik et al.[63]
dingthatsolubleKlothoand1,25(OH)2D
nd FGF23 levels increase in the early
nd that PTH levelsincreasein themore
Akimoto et al. [64] haverecently shown
Klotho levels of CKD patients, rather
Klotholevels,arelinked totheir number
phrons.Sakan et al.[65] recentlyreport-
renal α-Klotho levelsweresignificantly
um FGF23 levels were significantly ele-
d intermediate CKD, serum P levelsre-
he normal range. Despite falling renal
heincreasein FGF23 enhanced urinary
d serum 1,25(OH)2D levelsin early and
D, though not in advanced CKD. In ad-
ubleKlotho levelsfell significantly over
overlapping distinct mechanisms of initiation and pro-
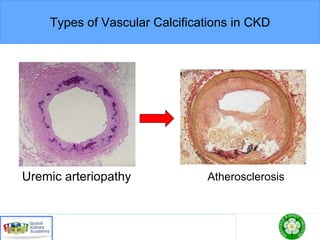
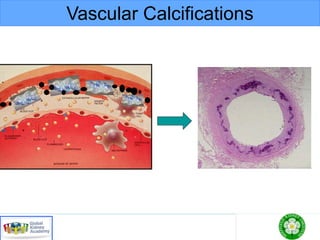
gression [68, 69].Vascular calcification isadynamicpro-
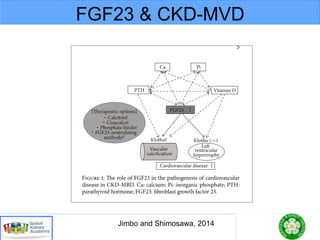
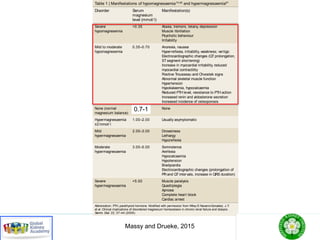
Fig. 5. Timeprofileof changesinplasmaFGF23,Klotho,activevi-
taminD,andphosphatelevelsasCKDprogresses. Thedecreasein
Klothoproteininthebloodisanearlyevent inCKDandisprogres-
sivelyreducedalongwiththedeclineof renal function.LowKlotho
partiallyinducesFGF23resistance,causinganinitial compensatory
increasein blood FGF23tomaintain Phomeostasis. Theincrease
inFGF23decreasesactivevitaminDlevelsandisfollowedbyeleva-
tion of PTH. Hyperphosphatemia is relatively late event in ad-
vancedCKD[reprintedwithpermissionfrom 60].
Colorversionavailableonline](https://image.slidesharecdn.com/ckdmbdgcc2017final2-190412163306/85/CKD-MBD-2017-63-320.jpg)
![FGF23 and CKD
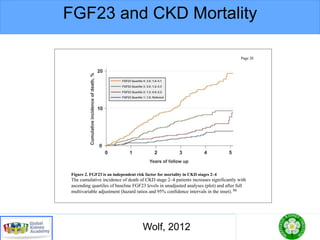
havebeen found to predict mortality not only among di-
alysispatientsbut amongpredialysisCKD patientsaswell
[22].
tial to facilitate thebinding of FG
The potential role of soluble Klo
in vivo remainsunknown at this
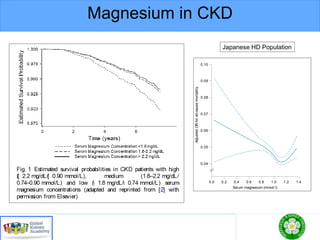
Fig. 2. Plasma FGF23 levels in thefour CKD stage groups. Boxes
represent the interquartile range with the upper and lower edges
representing the75th and 25th percentiles, respectively. Thereisa
statistically significant linear increase in plasma FGF23 levels
acrossthefour CKD groupsdivided by eGFR[reprinted with per-
mission from 21].
Fig. 3. Klotho family showing theth
themammalian genome. Homologo
mainsareconserved. Solubleformso
byalternativesplicingof itstranscrip
of thetransmembraneformbyβ-secr
Colorversionavailableonline](https://image.slidesharecdn.com/ckdmbdgcc2017final2-190412163306/85/CKD-MBD-2017-65-320.jpg)