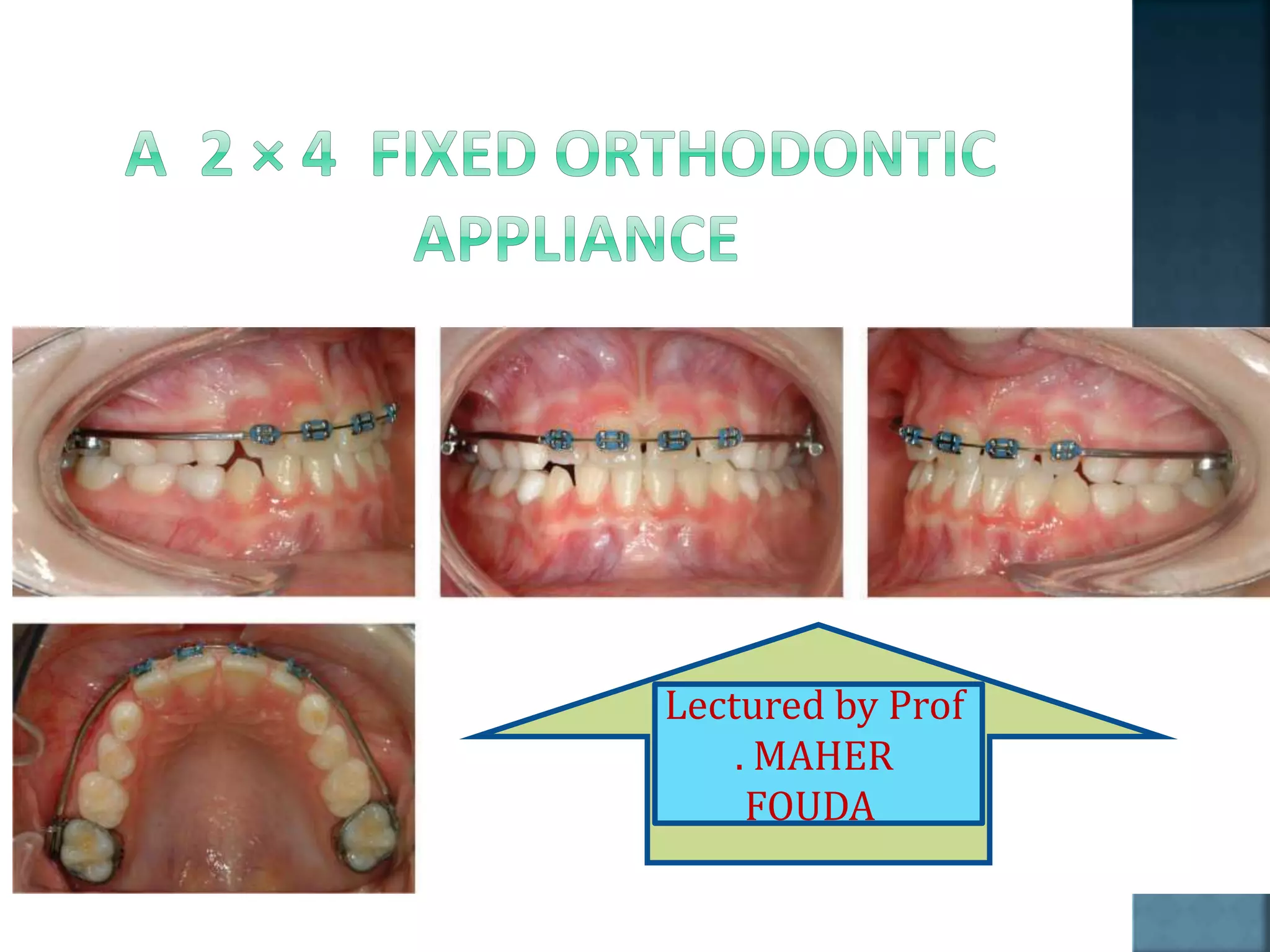
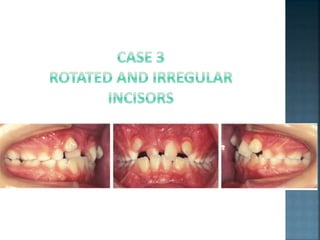
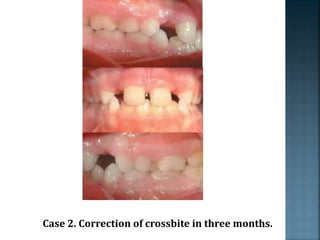
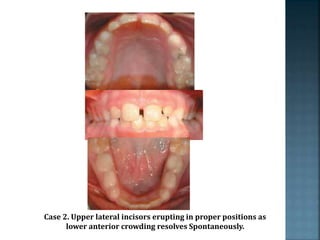
This document discusses the use of fixed 2x4 appliances to correct anterior crossbites in the mixed dentition. Key points include:
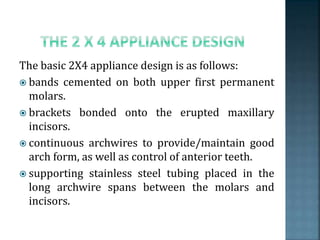
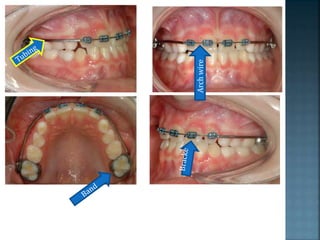
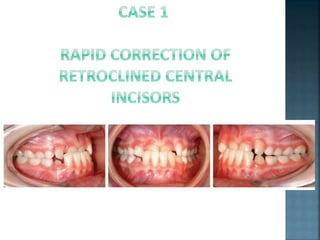
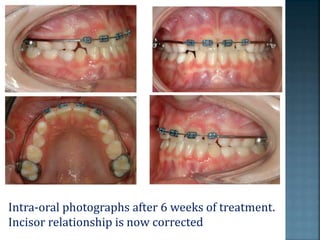
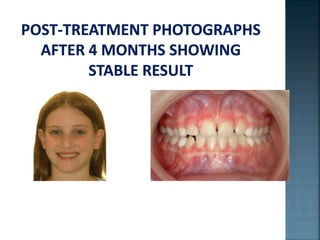
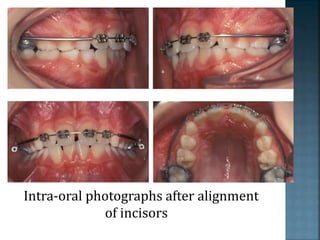
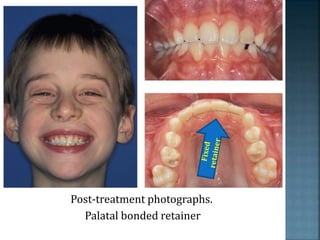
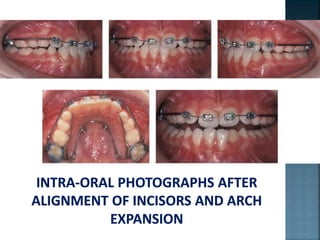
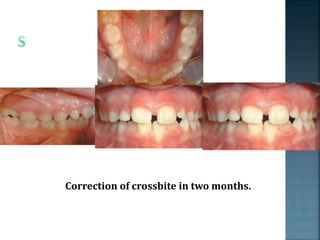
- Bands are placed on upper first molars and brackets bonded to incisors with an initial aligning wire. Crossbites can often be corrected within a few weeks.
- Factors like displacement, tooth damage, space issues and developing permanent teeth are considered before treatment.
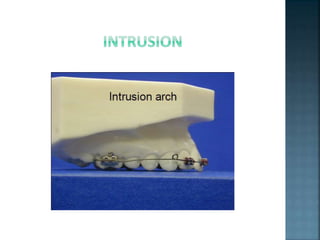
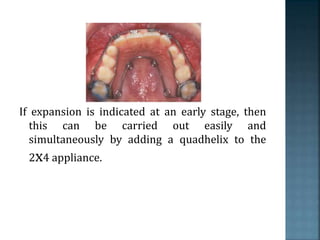
- A quadhelix can be added for minor expansion if needed. Fixed appliances allow for better control of forces compared to removable appliances.
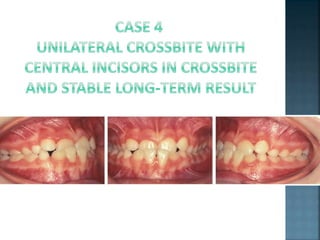
- Causes of crossbites include trauma, extractions, retained teeth and supernumeraries.
- Advantages of fixed appliances










































































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





