Download to read offline
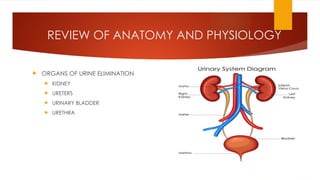










The document covers urinary elimination and bowel elimination, highlighting anatomy, physiology, urine composition, and factors influencing urination and defecation. It discusses types of urine specimens, collection methods, catheterization procedures, and signs of alterations in urinary and bowel elimination. The document also outlines factors affecting both urinary and bowel processes, including diet, age, medications, and psychological influences.














































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)








![APPROACH TO FEVER IN PEDIATRICS[1].pptTT](https://cdn.slidesharecdn.com/ss_thumbnails/approachtofeverinpediatrics1-260125081456-d559e079-thumbnail.jpg?width=640&height=640&fit=bounds)