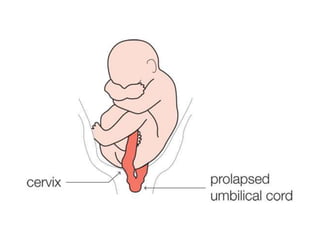
Umbilical cord prolapse is a rare obstetric emergency occurring when the umbilical cord slips ahead of the presenting part of the fetus, possibly leading to fetal distress or death. There are three types of cord prolapse—overt, occult, and funic presentation—and it is most common in cases of ruptured membranes or multiple births. Management includes various maneuvers or surgical intervention, with the highest incidence occurring in singleton pregnancies and risks associated with factors like malpresentation and excessive amniotic fluid.