Downloaded 60 times
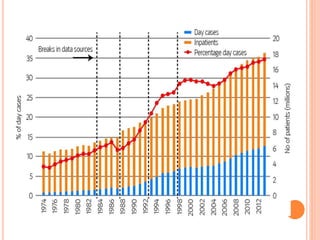











This document discusses day case surgery (DCS). It begins with an introduction on the prevalence of DCS internationally. It then covers the definition, history, merits and demerits of DCS. Key aspects of setting up and running a successful DCS unit are described, including space requirements, staffing, suitable procedures, pre-op preparation, and discharge criteria. The document concludes with a discussion on audit and special considerations for DCS in children and emergencies.






























![DAY_CARE_SURGERY[249].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/daycaresurgery249-230308170338-1755c0d8-thumbnail.jpg?width=640&height=640&fit=bounds)














































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)






