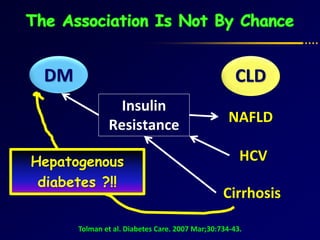
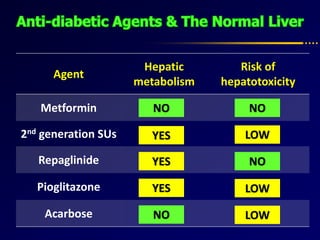
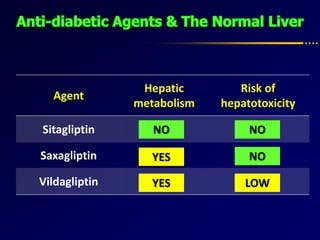
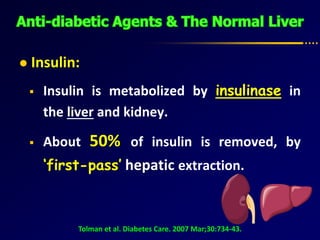
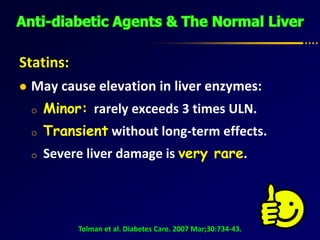
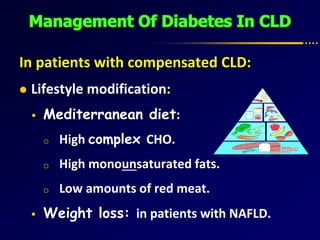
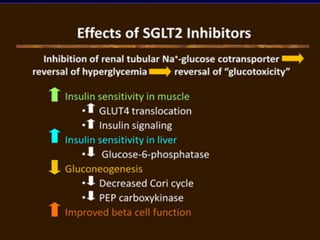
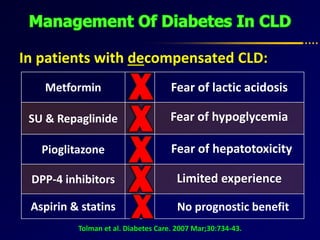
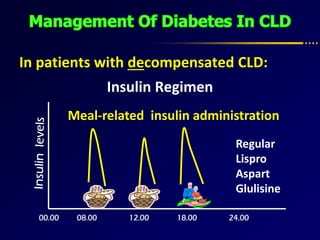
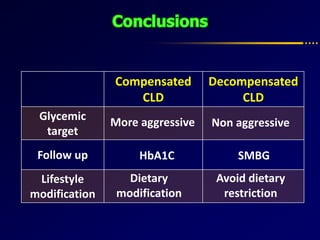
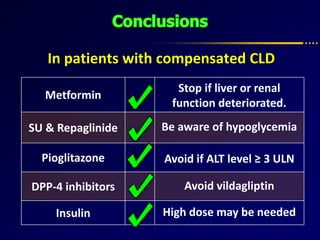
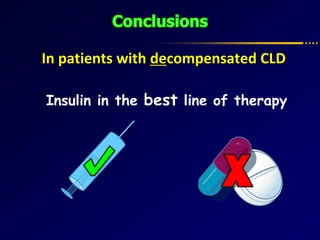
Diabetes and chronic liver disease (CLD) commonly coexist and interact with each other. CLD can cause abnormalities in glucose metabolism, while diabetes accelerates progression of CLD. For compensated CLD, anti-diabetic treatment is similar to those without liver disease. In decompensated CLD, tight glycemic control is not the goal and insulin therapy requires careful monitoring to avoid hypoglycemia due to altered liver function and insulin metabolism.

















![[2015] the treatment of diabetes mellitus of patients with chronic liver disease](https://cdn.slidesharecdn.com/ss_thumbnails/2015thetreatmentofdiabetesmellitusofpatientswithchronicliverdisease-151117004501-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)



























![Fatty liver disease with Diabetes Mellitus [BANGLADESH]](https://cdn.slidesharecdn.com/ss_thumbnails/fattyliverwithdmfinal-160520141759-thumbnail.jpg?width=640&height=640&fit=bounds)

























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






