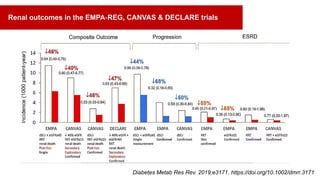
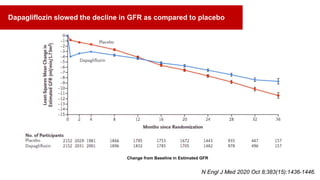
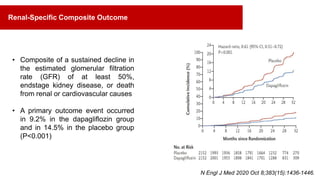
Dapagliflozin demonstrated clear treatment benefits for cardiovascular, kidney, and mortality outcomes in patients with chronic kidney disease (CKD), regardless of the presence of diabetes. It provides glomerular protection, limits proteinuria and kidney damage, and slows the decline of glomerular filtration rate in CKD patients. The DAPA-CKD trial found that dapagliflozin reduced the risk of end-stage renal disease or death from renal causes compared to placebo in CKD patients with and without type 2 diabetes. Dapagliflozin is indicated for the treatment of CKD up to stage III and was well tolerated with a low rate of treatment discontinuation.


















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



