Downloaded 275 times


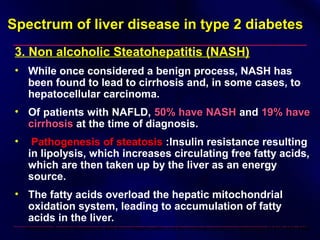




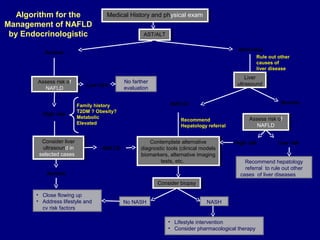
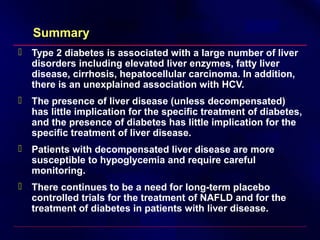


This document discusses the management of diabetes in patients with concomitant liver disease. It notes that about half of patients with cirrhosis have diabetes due to insulin resistance caused by the liver disease. Lifestyle changes and metformin are recommended initially if liver disease is mild. Insulin, sulfonylureas, meglitinides, alpha-glucosidase inhibitors, and thiazolidinediones may be used, with monitoring needed due to potential side effects or altered drug metabolism in liver disease. Insulin requirements can vary depending on the stage of liver disease.

![Fatty liver disease with Diabetes Mellitus [BANGLADESH]](https://cdn.slidesharecdn.com/ss_thumbnails/fattyliverwithdmfinal-160520141759-thumbnail.jpg?width=640&height=640&fit=bounds)

![[2015] the treatment of diabetes mellitus of patients with chronic liver disease](https://cdn.slidesharecdn.com/ss_thumbnails/2015thetreatmentofdiabetesmellitusofpatientswithchronicliverdisease-151117004501-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)


























































































