This document provides information on the history and types of local anesthesia. It discusses key details such as:
- Carl Koller demonstrated the first clinical use of local anesthesia in 1884 using procaine. Lidocaine was developed in 1948 and widely used.
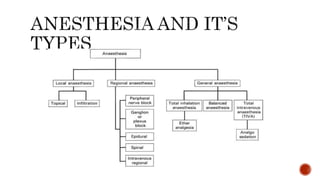
- Local anesthesia involves topical anesthetics or local infiltration of drugs like lidocaine to numb circumscribed body areas.
- Common uses are for excision procedures, dentistry work, dermatology procedures and biopsies. Potential risks include infection, hematoma, and nerve damage.






































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)






