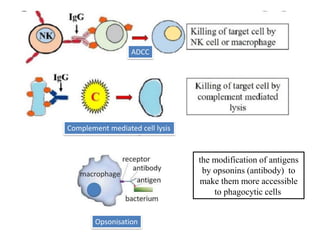
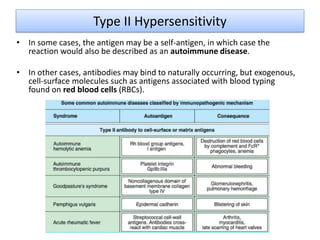
Type II hypersensitivity is an antibody-mediated immune reaction involving IgG and IgM antibodies that damage cells by targeting their antigens, leading to conditions such as transfusion reactions and autoimmune diseases. The reaction occurs in two phases: sensitization, where antibodies are produced, and effector, where destruction of target cells is executed via complement activation, antibody-dependent cell-mediated cytotoxicity, or opsonization. Immediate hypersensitivity reactions can cause severe complications, including shock and multi-organ failure.