Process of Triage’s Assessment 1.Across the room assessment 2. Triage physical assessment 3.Triage history 4.Triage decision
4.
Across the roomassessment A – Airway status B – Breathing status C – Circulatory status D - Disability
5.
Triage Physical Assessmentเป้าหมาย : ประเมินได้ครอบคลุม + ซักประวัติอย่างย่อๆ หัวข้อในการซักประวัติ : O L D C A R T O : Onset of symptom L : Location Of Problem C : Characteristics the patient uses to describe the symptom D : Duration of symptom A : Aggravating factors R : Relieving factors T : Treatment administered before arrival
6.
Triage History CI A M P E D S C : Chief complaint I : Immunization A : Allergies M : Medication P : Past medical history E : Events surrounding D : Diet S : Symptom
7.
Triage Decision 1.Immediately life-threatening : 1A or 1B 1A : multiple trauma + life threatening 1B : life threatening 2. Imminently life threatening 3. Potential life-threatening 5. Least urgent 4. Potential serious Australasian Triage Scale : ATS
8.
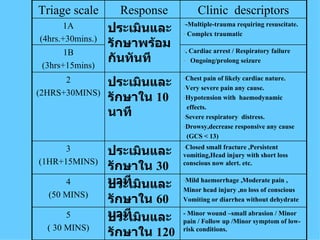
-Multiple-trauma requiring resuscitate.Complex traumatic ประเมินและรักษาพร้อมกันทันที 1A (4hrs.+30mins.) - Minor wound –small abrasion / Minor pain / Follow up /Minor symptom of low-risk conditions. ประเมินและรักษาใน 120 นาที 5 ( 30 MINS) Mild haemorrhage ,Moderate pain , Minor head injury ,no loss of conscious Vomiting or diarrhea without dehydrate ประเมินและรักษาใน 60 นาที 4 (50 MINS) Closed small fracture ,Persistent vomiting,Head injury with short loss conscious now alert. etc. ประเมินและรักษาใน 30 นาที 3 (1HR+15MINS) Chest pain of likely cardiac nature. Very severe pain any cause. Hypotension with haemodynamic effects. Severe respiratory distress. Drowsy,decrease responsive any cause (GCS < 13) ประเมินและรักษาใน 10 นาที 2 (2HRS+30MINS) . Cardiac arrest / Respiratory failure Ongoing/prolong seizure 1B (3hrs+15mins) Clinic descriptors Response Triage scale
9.
Process of Triage Nurse 1. Assessment 2. Priority of care ( Triage category ) 3. First aid 5. Public relations 6. Diagnostic , therapeutic intervention 4. Referral 7. Documentation