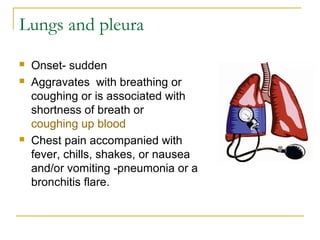
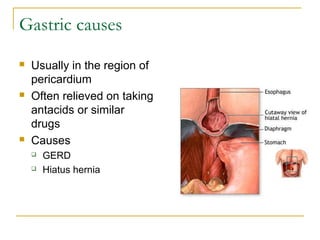
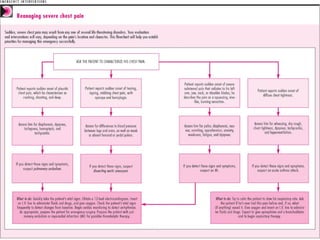


The document discusses various causes of chest pain, categorizing them into cardiac, pulmonary, gastrointestinal, and musculoskeletal sources, with detailed descriptions of symptoms and potential treatments. It highlights a case study of a stressed entrepreneur, Bob, whose chest pain was identified as atypical GERD symptoms after thorough cardiac examinations, leading to effective management with a PPI. The document emphasizes the importance of careful diagnosis and management of chest pain to alleviate patient anxiety and improve health outcomes.





































![[Int. med] chest pain 3rd year class](https://cdn.slidesharecdn.com/ss_thumbnails/int-150502144317-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Int. med] chest pain 3rd year class from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/zkh5x8lztsickjayhfry-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171705-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
















































