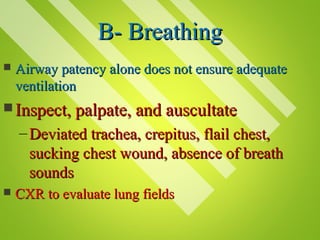
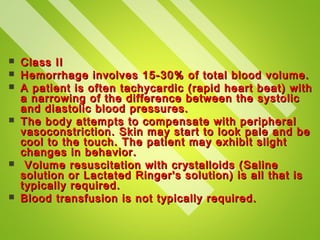
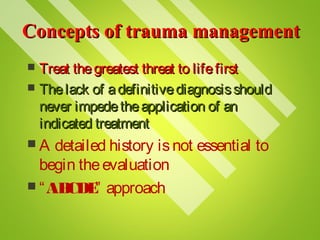
The document discusses the initial assessment and management of trauma patients. It outlines the ABCDE approach to prioritize airway, breathing, circulation, disability, and exposure. Specific interventions are described for addressing life-threatening injuries associated with each category. The goal is to rapidly identify and treat issues that pose the greatest risk to life, such as airway obstruction, tension pneumothorax, and hemorrhagic shock from blood loss.





![Pre-hospital triage
This triage of trauma patients usually depends on
three simple groups of factors:
Physiology: the vital signs (e.g. pulse >120/min,
systolic blood pressure <90 mmHg, Glasgow
Coma Scale score [GCS] <15)
Anatomy: the immediately evident injuries (e.g.
fractured long bones, spinal cord injury,
penetrating injury)
Mechanism of injury: e.g. fall >5 m, injury to
two or more body regions, vehicle crash with
ejection](https://image.slidesharecdn.com/trauma-130531054629-phpapp02/85/Trauma-8-320.jpg)