


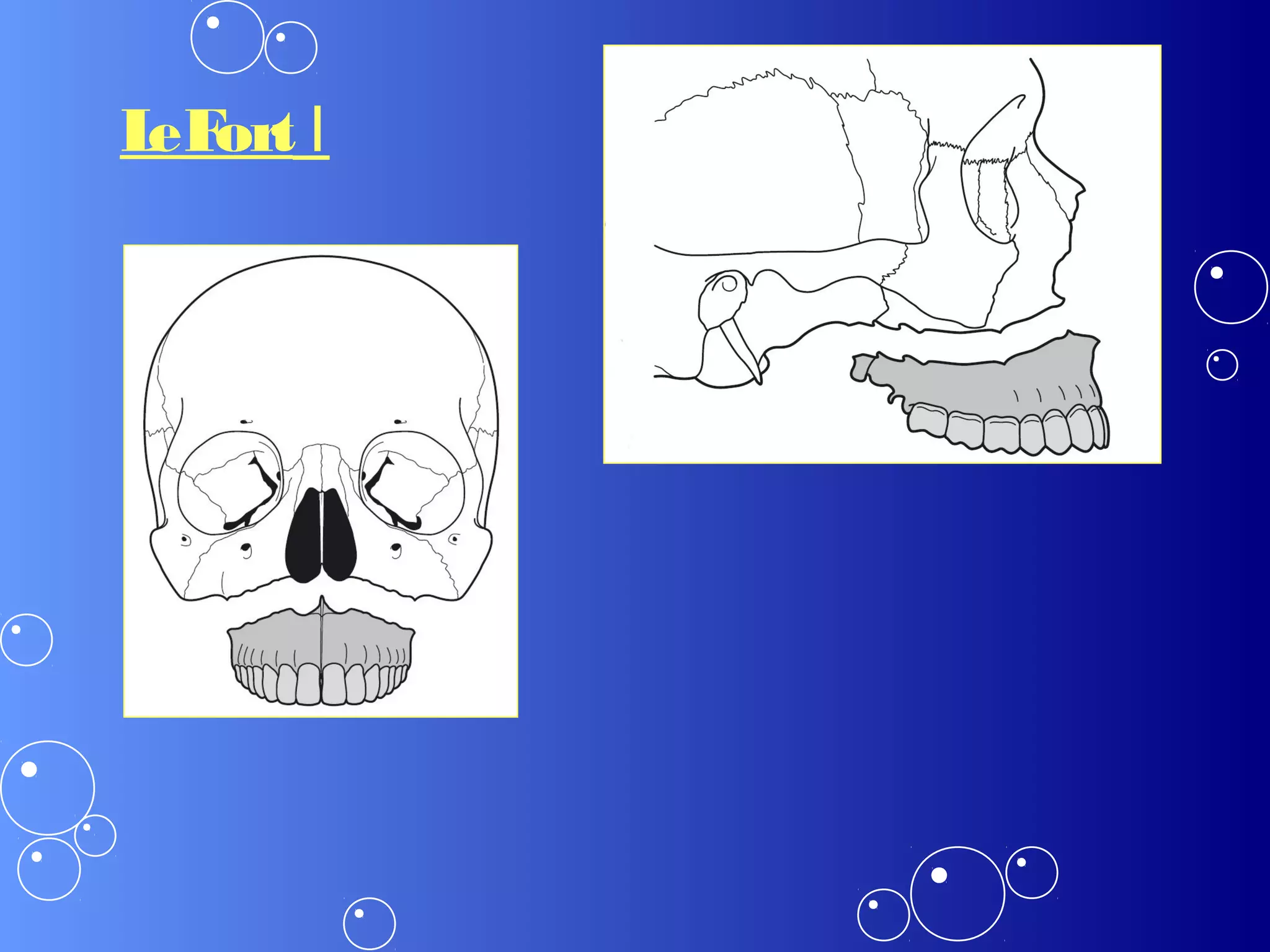
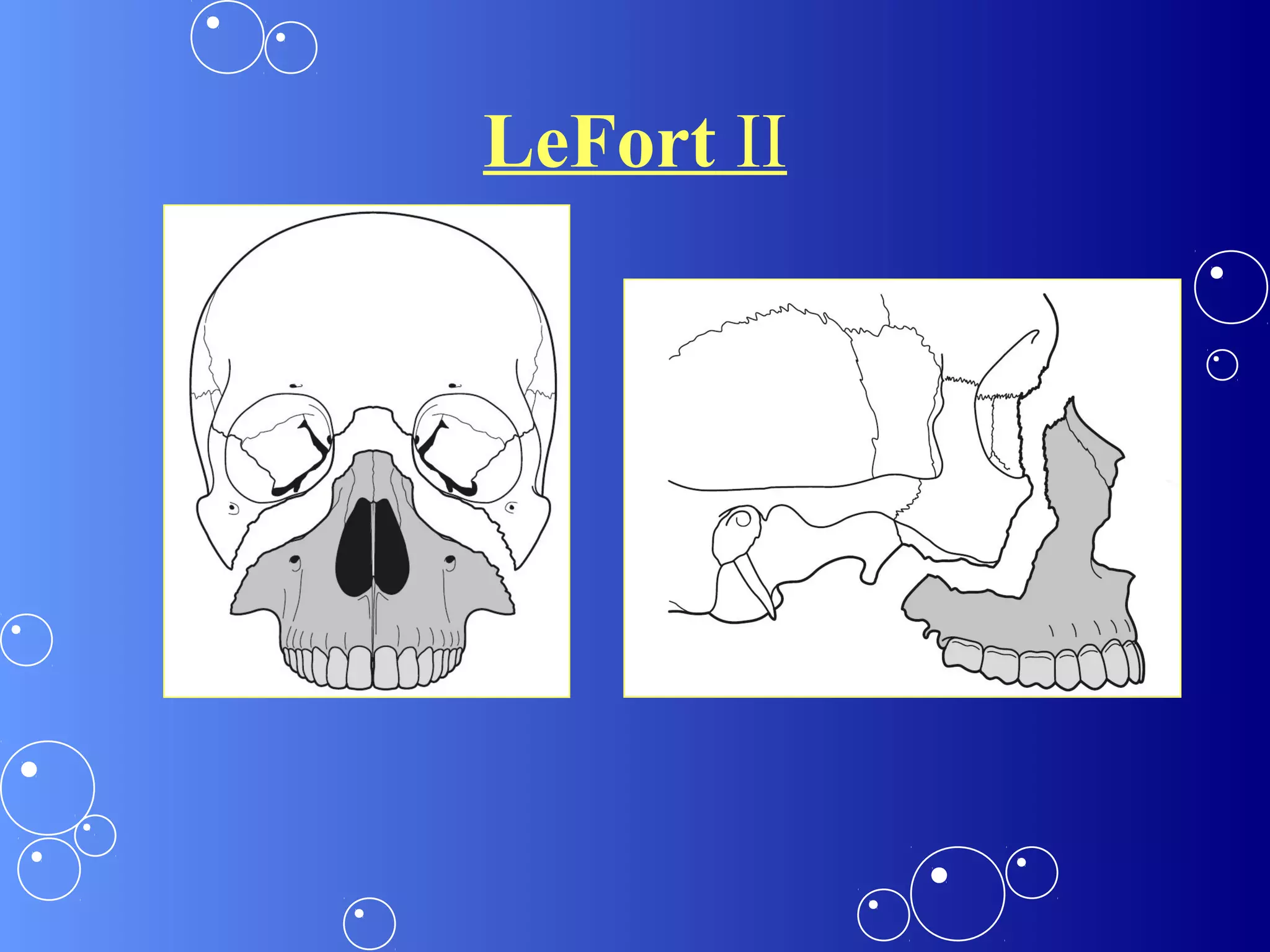
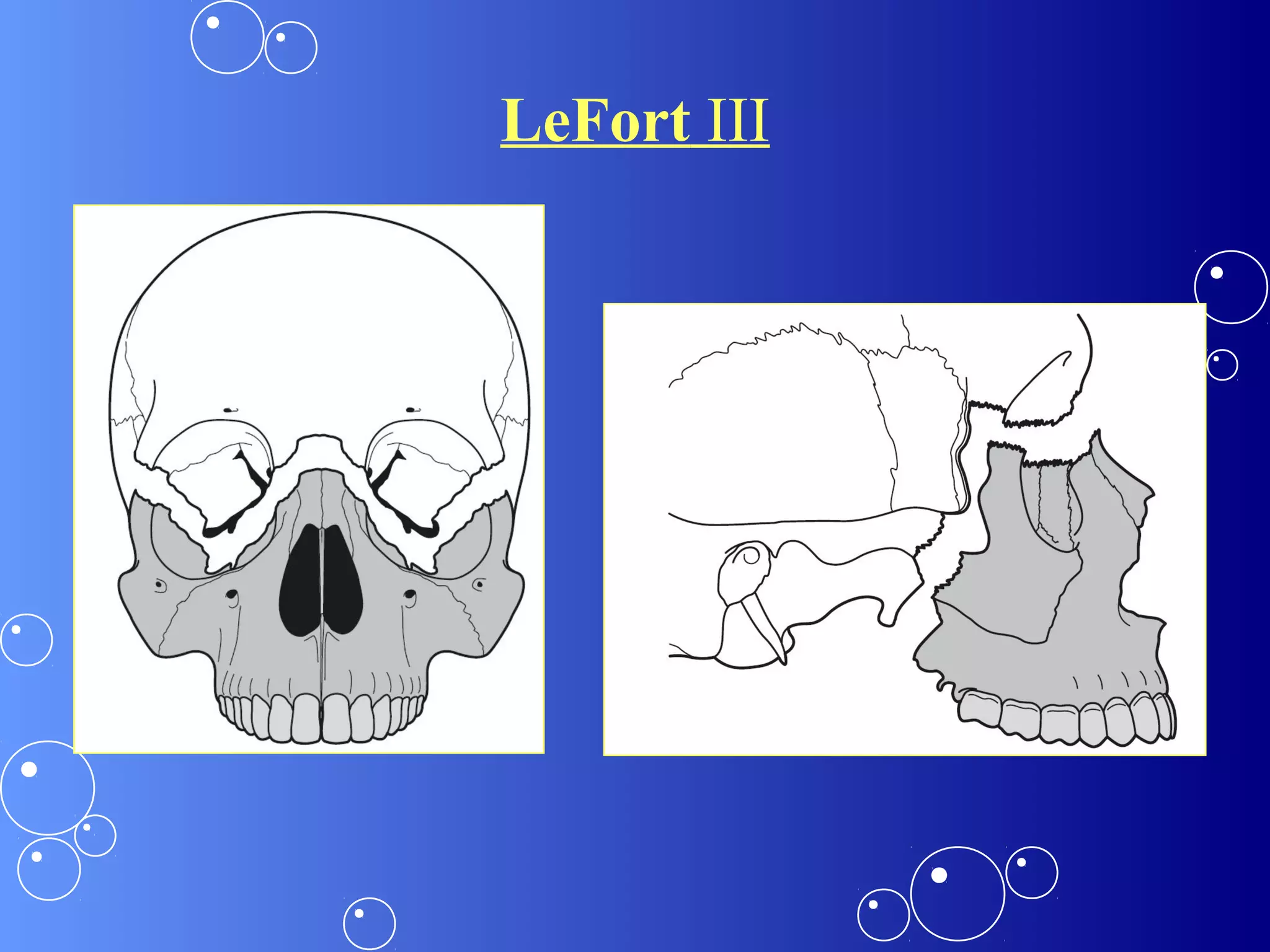


The document discusses maxillary fractures, their classification, and treatment. It notes that René LeFort classified maxillary fractures into 3 types based on the location of fracture lines. LeFort I involves the alveolar process, LeFort II the maxilla and nasal bones, and LeFort III separates the midface from the cranium. Treatment involves reduction using disimpaction forceps followed by fixation methods like wire osteosynthesis, rigid plates, or semi-rigid miniplates depending on the fracture type and location. Complications can include nerve damage, malocclusion, infection, and nonunion if not treated properly.













































































