Downloaded 667 times





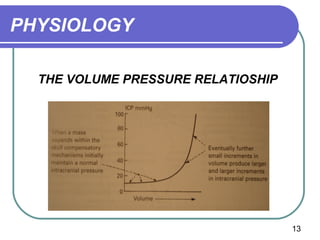






This document discusses increased intracranial pressure (ICP) by outlining the physiology of normal ICP and factors that increase ICP. It describes how the skull volume is occupied by brain, blood, and cerebrospinal fluid. Any increase in these contents can elevate ICP based on the Monroe-Kellie doctrine. Compensatory mechanisms aim to reduce ICP by decreasing CSF or blood volume, but herniation may occur if pressure rises beyond compensation. Clinical signs of increased ICP range from headache to herniation and death. Management focuses on reducing pressure through various medical or surgical interventions and monitoring ICP.