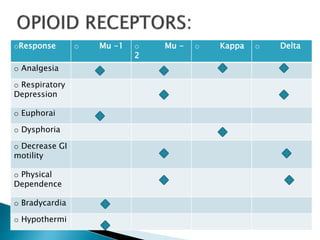
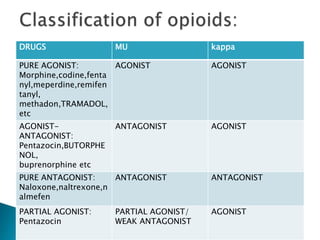
This document discusses opioid analgesics, focusing on tramadol and butorphanol. It defines opioids and their receptor types. Tramadol is described as a centrally acting atypical analgesic that is a racemic mixture with both enantiomers contributing to its analgesic effects. Its mechanisms of action and pharmacokinetics are outlined. Butorphanol is introduced as a synthetic agonist-antagonist opioid with greater agonist and antagonist effects than pentazocin. Its proposed mechanisms of analgesia and adverse effects are summarized. Clinical uses of both drugs for various acute and postoperative pain conditions are mentioned.





































































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)

















