This document provides information about total parenteral nutrition (TPN), including:
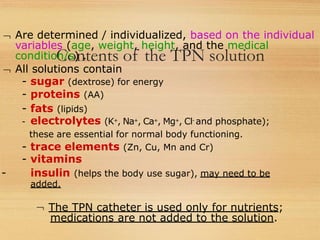
- TPN involves administering nutrients intravenously to bypass the digestive system for patients who cannot eat or absorb nutrients normally. It provides all necessary nutrients like glucose, proteins, fats, vitamins and minerals.
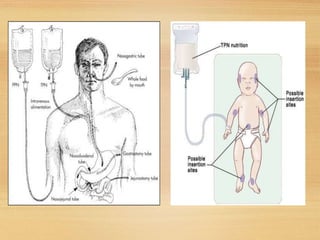
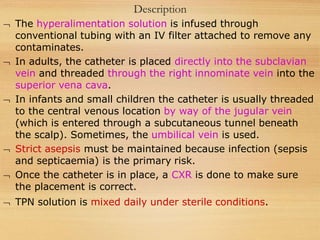
- A central venous catheter is surgically placed in a large vein like the superior vena cava to administer high volumes and concentrations of nutrients. Strict sterility must be maintained to prevent infection.
- TPN requires balancing the nutrients and monitoring the patient closely as metabolic and fluid imbalances can occur if not managed properly. It is a medical intervention used when enteral nutrition is not possible.
![Total Parenteral Nutrition
Also called central parenteral nutrition (CPN) or
‘hyperal’ (hyperalimentation).
[The term ‘hyperalimentation’ is a misnomer because it
incorrectly implies that nutrients are supplied in excess
of needs].
Large amounts of nutrients in a hypertonic solution can
be supplied via TPN. The catheter is surgically placed
into the superior vena cava.
The reason that larger amounts of nutrients in a
hypertonic solution can be supplied via the superior
vena cava than with peripheral parenteral nutrition is
that the superior vena cava has a much larger diameter
and a higher blood flow rate, both of which quickly
dilute the TPN solution.](https://image.slidesharecdn.com/totalparentralnutrition2-220531100841-f3a6b4a0/85/Total-Parentral-Nutrition-2-pptx-3-320.jpg)
![Purposes
Used when individuals cannot or should not get
their nutrition through eating.
Used when the intestines are obstructed, when the
small intestine does not absorb nutrients properly,
or a GI fistula (abnormal connection) is present.
To ensure ‘Bowel rest’ (food does not pass through
the bowels).
[Bowel rest may be necessary in Crohn's disease,
pancreatitis, ulcerative colitis, and with prolonged
bouts of diarrhea in young children].](https://image.slidesharecdn.com/totalparentralnutrition2-220531100841-f3a6b4a0/85/Total-Parentral-Nutrition-2-pptx-11-320.jpg)
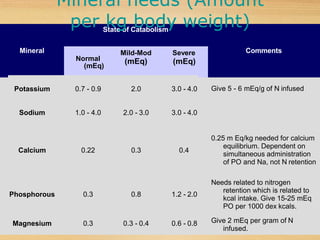
![Contents of the TPN solution (contd.)
For Adults: approx. 2 lts of TPN solution daily (varies
with the individual’s age, size and health).
The solution should be allowed to be warmed to room
temperature before intravenous nutrition begins. The
solution is infused slowly at first to prevent fluid
imbalances, then the rate is gradually increased. The
infusion process takes several hours.
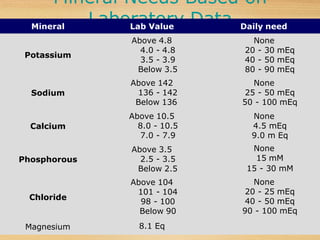
Successful TPN requires frequent, often daily
monitoring of the individual's parameters [weight,
glucose levels, FBC, blood gasses, fluid balance, urine
output, waste products in the blood (plasma urea);
electrolytes];
LFT & RFT may also be performed (special cases).](https://image.slidesharecdn.com/totalparentralnutrition2-220531100841-f3a6b4a0/85/Total-Parentral-Nutrition-2-pptx-18-320.jpg)