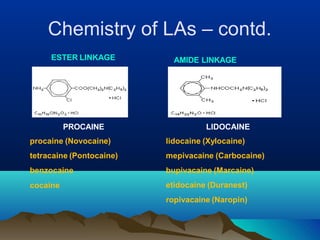
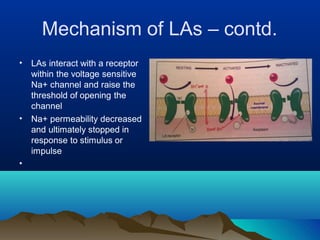
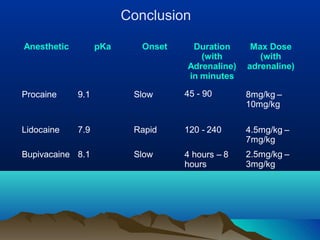
Local anesthetics are drugs that reversibly block nerve impulses and sensation of pain in localized areas. They work by inhibiting sodium influx through voltage-gated sodium channels in neurons. Common examples include lidocaine, bupivacaine, and tetracaine. Esters like procaine have a short duration due to rapid metabolism, while amides like lidocaine and bupivacaine have a longer duration due to liver metabolism. Local anesthetics are used topically, for infiltration, in spinal or epidural spaces, and for regional nerve blocks to provide anesthesia for various procedures.













































































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)






![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)




