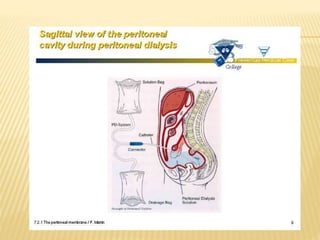
Peritoneal dialysis (PD) is a treatment for severe chronic kidney failure that uses the peritoneum in the abdomen as a membrane to exchange fluids and dissolved substances between the blood and dialysis fluid introduced into the abdomen. Fluid is introduced through a permanent abdominal catheter and removed periodically, either continuously throughout the day or automatically at night. PD provides an alternative to hemodialysis by allowing treatment without visiting a medical facility but carries risks like infection from the permanent catheter. Nursing management of PD includes monitoring for complications, supporting nutrition, managing discomfort, and providing health teaching.






























![Growth And Development During Early Childhood[1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/growthanddevelopmentduringearlychildhood1-241018102522-364de685-thumbnail.jpg?width=640&height=640&fit=bounds)





![Growth And Development During Early Childhood[1].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/growthanddevelopmentduringearlychildhood1-240428175610-ceeff808-thumbnail.jpg?width=640&height=640&fit=bounds)


























![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





