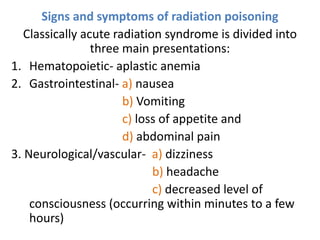
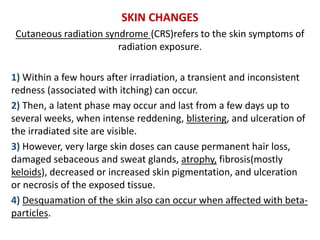
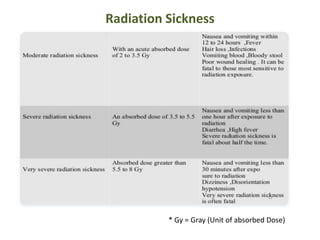
This document discusses radiation poisoning and its effects. It begins by defining radiation and its sources, both natural and synthetic. It then defines radiation poisoning, also known as radiation sickness, and classifies radiation as either ionizing or non-ionizing. Ionizing radiation can damage DNA and cells by removing electrons. Exposure effects depend on dose and duration, and can be immediate, chronic, or delayed. Symptoms of radiation poisoning are discussed for different organ systems. Prevention, diagnosis, and treatments such as decontamination, supportive care, and medications like potassium iodide and filgrastim are summarized.




![IR Sources and Effects
Sources - Most are thermal sources (plasma torches,
halogen lamps)
• Target Organs : skin and eyes
• Can damage : cornea, iris, retina and lens of the eye
• Skin : heats/burn surface of the skin and tissues
Biological Effects [Microwaves]
• Primarily thermal effects
• cataracts , biochemical changes
• Secondary problems (pace-makers, etc.)
• The latter are also capable of disrupting the normal
function of electronic medical devices such as
subcutaneously implanted cardiac pacemakers and
monitors.](https://image.slidesharecdn.com/radiationpoisoning1-220330144751/85/RADIATION-POISONING-1-pptx-26-320.jpg)
![B) Internal decontamination
• Some treatments may reduce damage to internal organs
caused by radioactive particles.
• Ingested radioactive material should be removed promptly
by induced vomiting or lavage if exposure is recent.
• Frequent mouth rinsing with saline or dilute hydrogen
peroxide is indicated for oral contamination.
• Exposed eyes should be decontaminated by directing a
stream of water or saline laterally to avoid contaminating
the nasolacrimal duct
• Saturation of the target organ (e.g., potassium iodide [KI]
for iodine isotopes)
• Chelation at the site of entry or in body fluids followed by
rapid excretion (e.g., calcium or zinc diethylene triamine
penta acetate [DTPA] for americium, californium,
plutonium, and yttrium)](https://image.slidesharecdn.com/radiationpoisoning1-220330144751/85/RADIATION-POISONING-1-pptx-32-320.jpg)
![Treatment for damaged bone marrow
A protein called granulocyte colony-stimulating factor,
which promotes the growth of white blood cells, may
counter the effect of radiation Sickness on bone marrow.
Treatment with this protein-based medication, which
includes filgrastim (Neupogen), and pegfilgrastim
(Neulasta), may increase white blood cell production and
help prevent subsequent infections.
10 mcg/kg SC as a single daily injection for patients
exposed to myelosuppressive doses of radiation.
Administer as soon as possible after suspected or
confirmed exposure to radiation doses > 2 grays (gy).
Sargramostim (granulocyte macrophage colony-
stimulating factor [GM-CSF]) 5 to 10 mcg/kg sc once/day
or 200 to 400mcg/m2 sec once/day.](https://image.slidesharecdn.com/radiationpoisoning1-220330144751/85/RADIATION-POISONING-1-pptx-37-320.jpg)