Downloaded 10 times




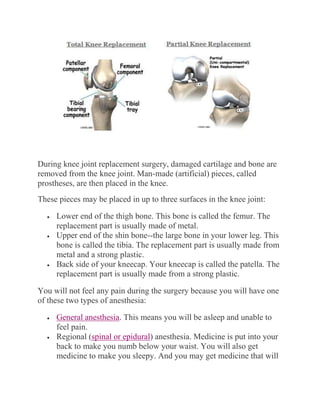












Osteoarthritis is a degenerative joint disease that commonly affects weight-bearing joints like the knee and hip. It has multiple causes but is generally attributed to normal wear and tear over time. Knee osteoarthritis symptoms include pain, swelling, stiffness, and reduced mobility. Treatments include medications, physical therapy, bracing, and knee replacement surgery for severe cases. Knee replacement surgery involves removing damaged bone and cartilage and replacing them with artificial implants. Extensive physical therapy is then needed for rehabilitation and recovery of strength and mobility.



































































