Downloaded 31 times


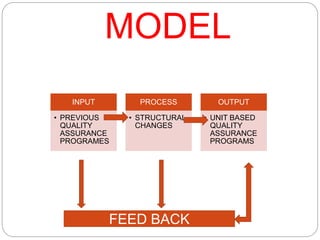
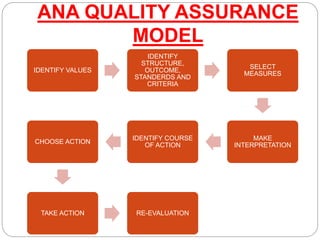

This document discusses quality assurance in healthcare and the role of nurses. It defines quality and quality assurance, and outlines some models for quality assurance programs. Key points include: - Quality assurance aims to systematically review, analyze, and evaluate compliance with standards to ensure quality of care. - Components of quality healthcare include professionalism, efficient resource use, low patient risk, patient satisfaction, and positive health outcomes. - Nurses play an important role in quality assurance through participation in quality improvement teams, monitoring care effectiveness, innovation, patient safety initiatives, education, and research. - Common models for quality assurance programs include the system model, ANA model, JCAHO model, and ISO model. These aim






































































