Downloaded 865 times

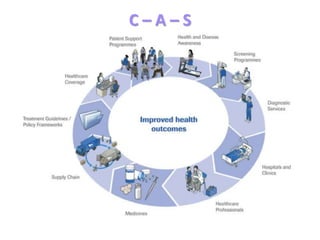
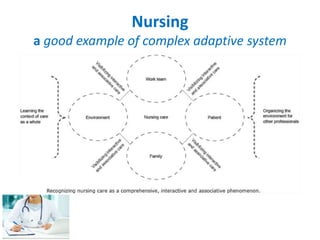


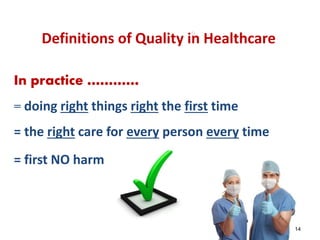
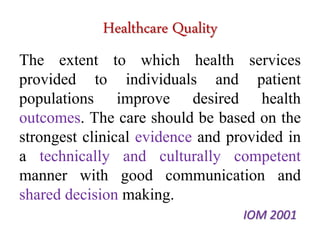




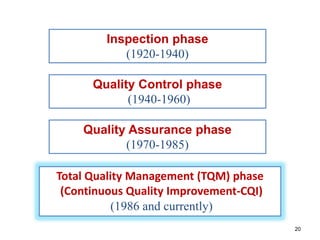





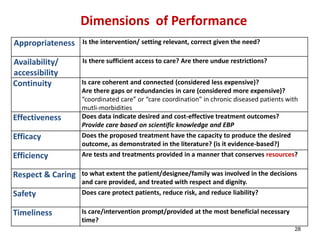
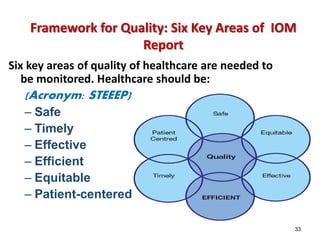









The document outlines fundamental concepts of healthcare quality, emphasizing the need for continuous improvement and adherence to established standards to enhance patient outcomes. It discusses various dimensions of healthcare quality, including safety, effectiveness, and patient-centered care, while referencing the IOM's aims for a high-performing healthcare system. The content aims to educate participants on the complexities and evolving standards within healthcare to meet rising demands and improve system performance.







































































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)














