Download as PDF, PPTX
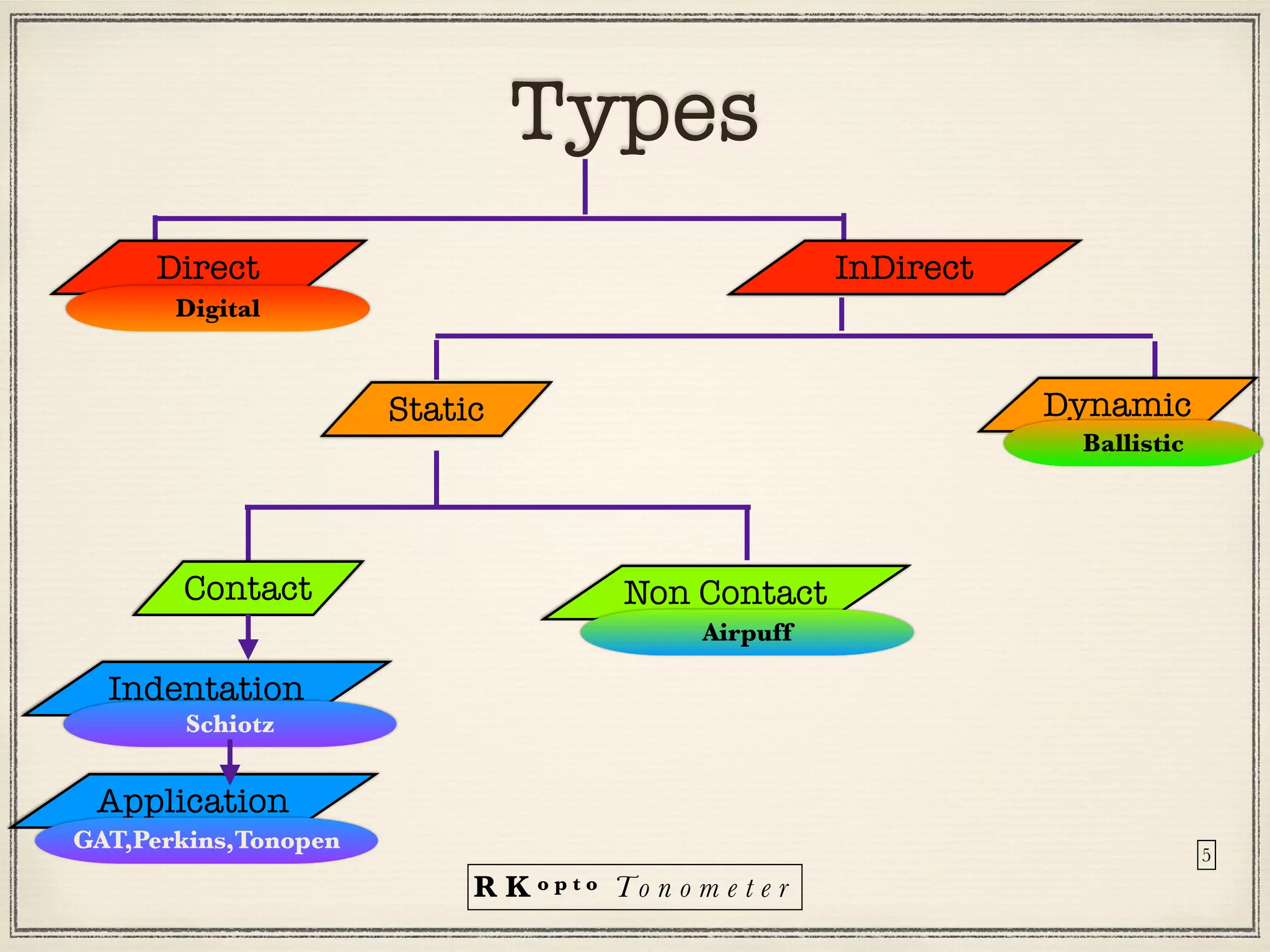
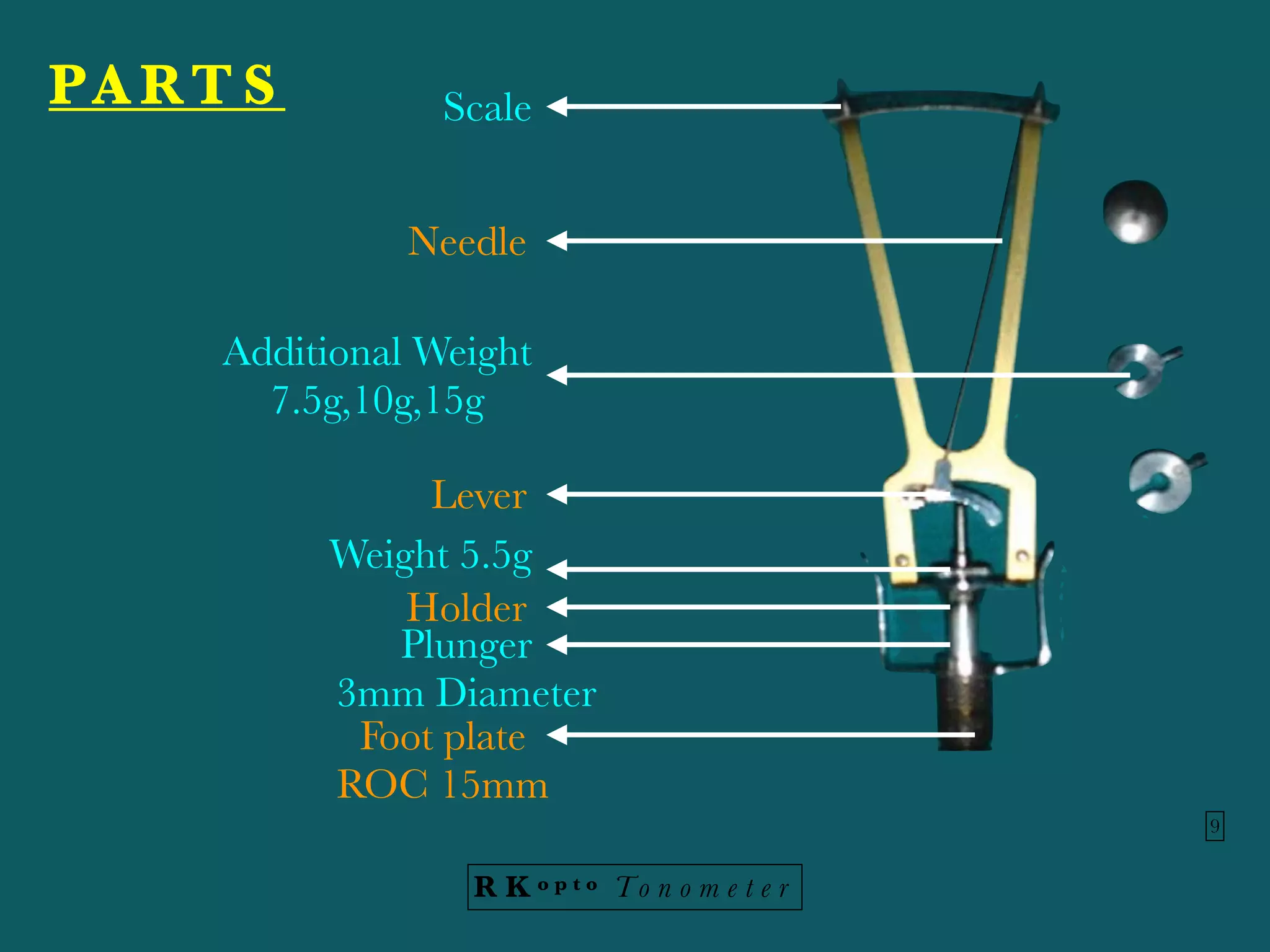

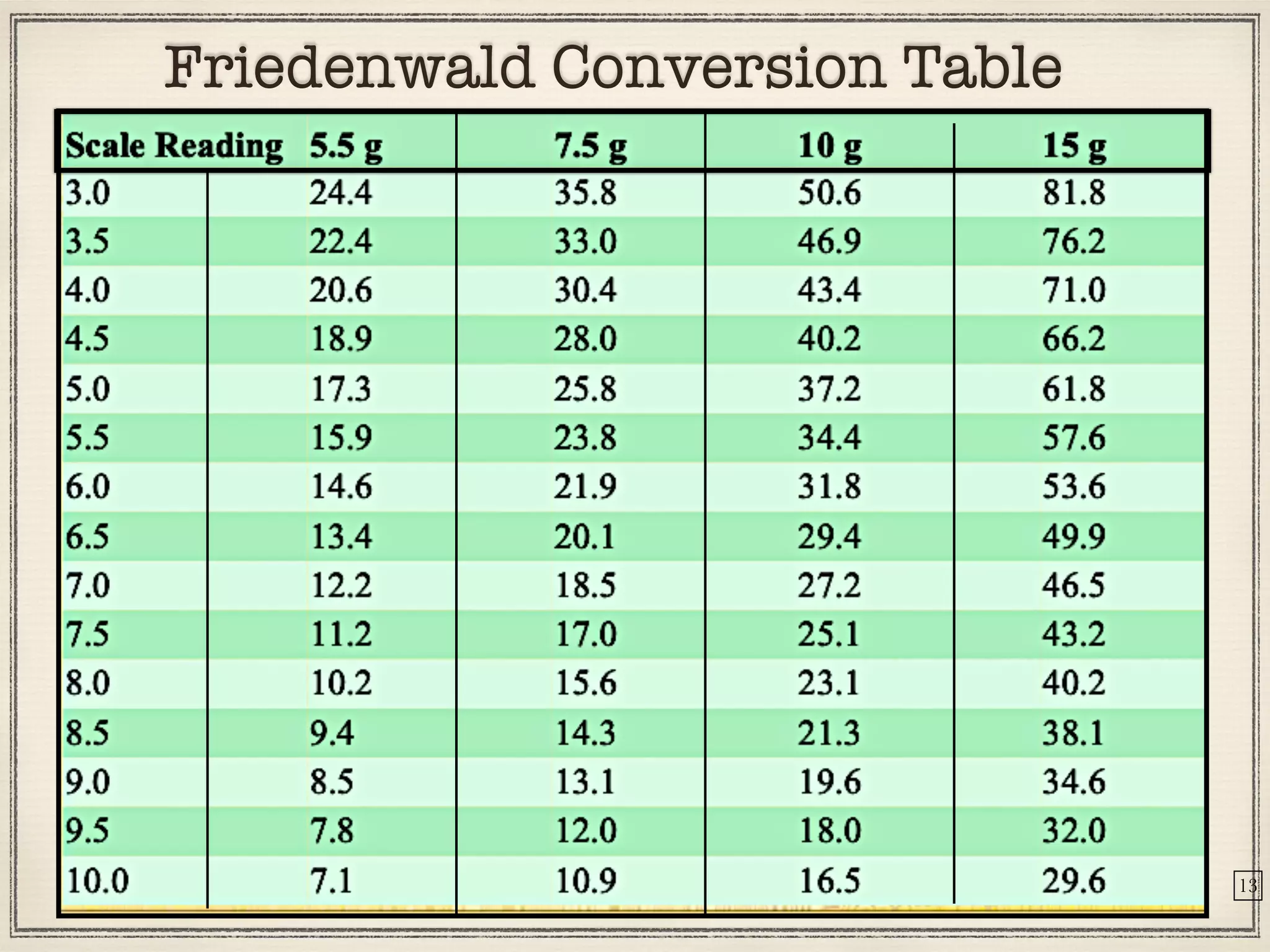









Tonometers are devices used to measure intraocular pressure (IOP) for assessing eye health, with a history spanning from 1826 to modern digital devices. Various types include direct, indirect, contact, and non-contact tonometers, each with unique characteristics and calibration methods. The document outlines procedures, advantages, limitations, and specifications for tonometers, emphasizing the significance of accuracy and proper use in clinical settings.



































































