Downloaded 27 times

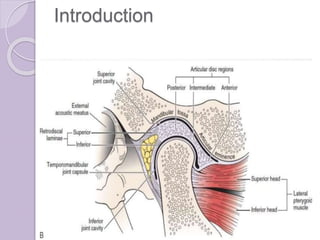
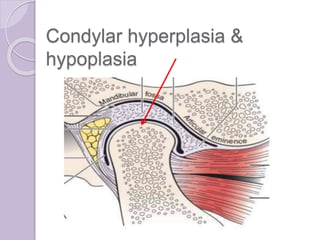
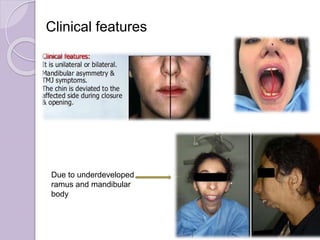
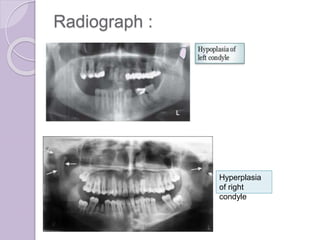

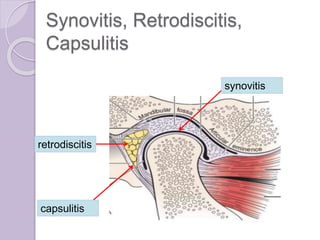













The document discusses temporomandibular joint (TMJ) disorders, including their classification, causes, and clinical features. It covers specific conditions such as condylar hypoplasia/hyperplasia, synovitis, disc derangement, various types of arthritis affecting the TMJ, and associated pain dysfunction syndromes. Management and treatment options for these disorders, including surgical and conservative methods, are also outlined.






























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)




