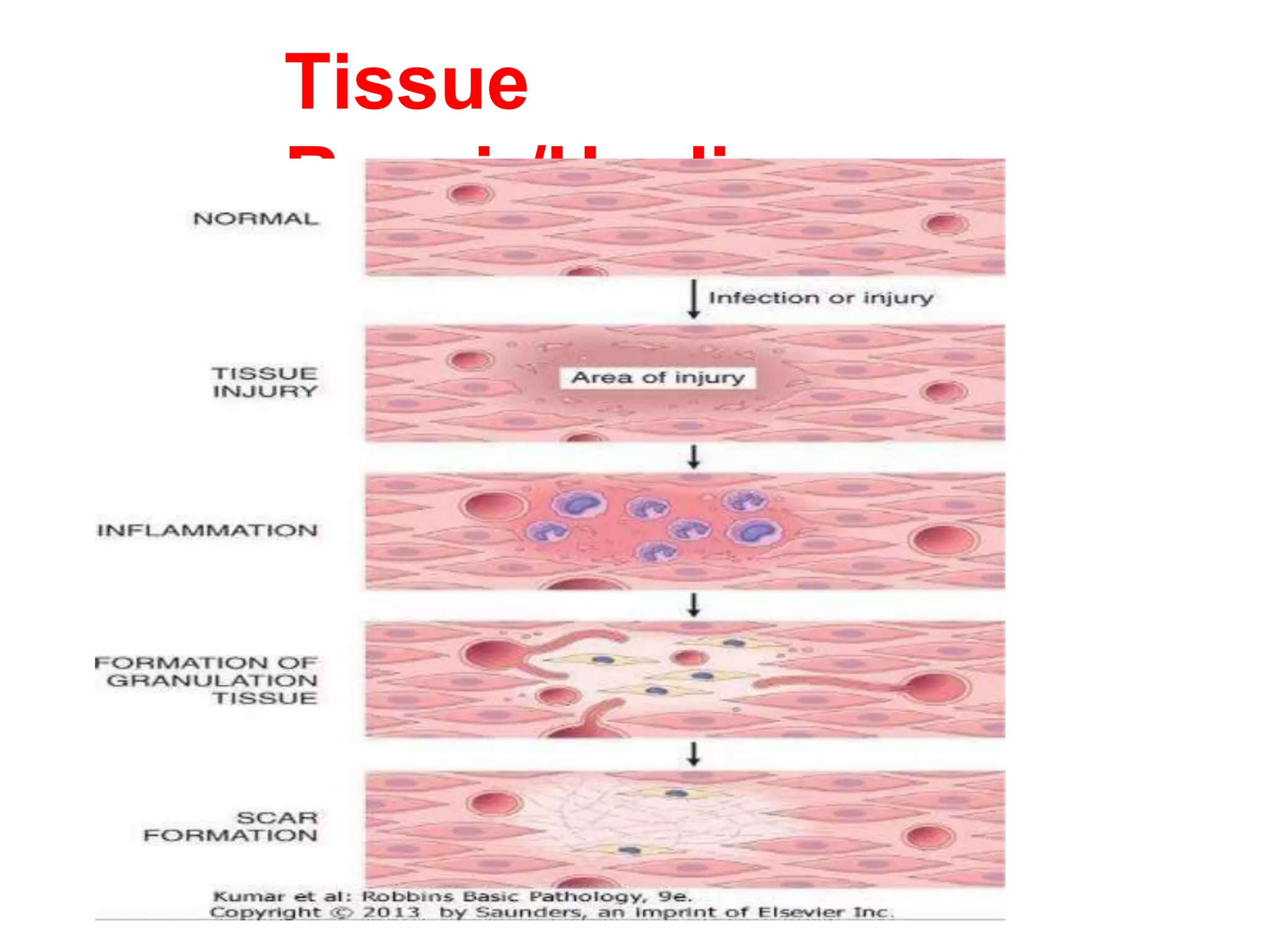
Tissue repair occurs through two main processes: regeneration and scar formation. Regeneration involves the proliferation of residual cells to completely restore lost tissue, while scar formation deposits connective tissue when regeneration is not possible. Wound healing involves inflammation, proliferation, granulation tissue formation, wound contraction, and strength acquisition. Tissue repair is influenced by factors like nutrition, infection, and wound location. Complications can arise from deficient or excessive scar formation, exuberant granulation tissue, and contractures.