1. Mycobacterium tuberculosis enters macrophages and replicates within phagosomes, inhibiting phagolysosome fusion.
2. A TH1 immune response is mounted after 3 weeks of infection to activate macrophages. IFN-γ is critical for macrophage activation.
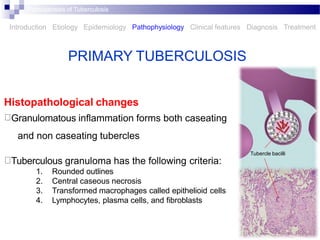
3. Granulomatous inflammation forms caseating and non-caseating tubercles containing central necrosis, epithelioid cells, and lymphocytes. Tuberculosis may not elicit granulomas in immunosuppressed individuals.




![EPIDEMIOLOGY
Roughly one of every three people on earth is infected by
M. tuberculosis
The distribution is very uneven, with the highest incidences
found in southern Asia and sub-Saharan Africa
In the United States, about 13 million people have LTBI,
evidenced by a positive skin test [purified protein derivative
(PPD)] but no signs or symptoms of disease
Pathogenesis of Tuberculosis
Introduction Etiology Epidemiology Pathophysiology Clinical features Diagnosis Treatment](https://image.slidesharecdn.com/tuberculosis2-221230060459-53be84c9/85/tuberculosis-2-pptx-5-320.jpg)