Download as PDF, PPTX

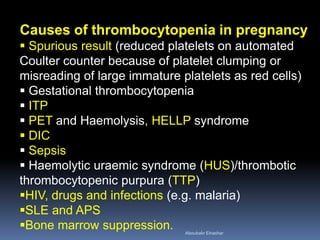
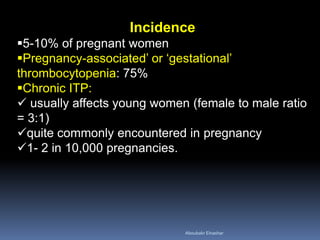
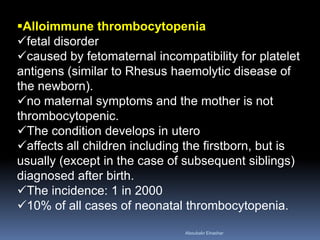

This document discusses thrombocytopenia during pregnancy. It defines the causes as gestational thrombocytopenia, ITP, preeclampsia, infections, and other conditions. For ITP, it describes the pathogenesis as autoantibodies destroying platelets and diagnoses it through excluding other causes. It notes ITP has little effect on pregnancy but the risk of fetal thrombocytopenia is around 5-10%. Management involves monitoring platelet counts and treating if needed before delivery or if bleeding occurs, using corticosteroids or IVIG as first-line therapies. The neonatal risks are also low if platelet counts are monitored after birth.











































































































