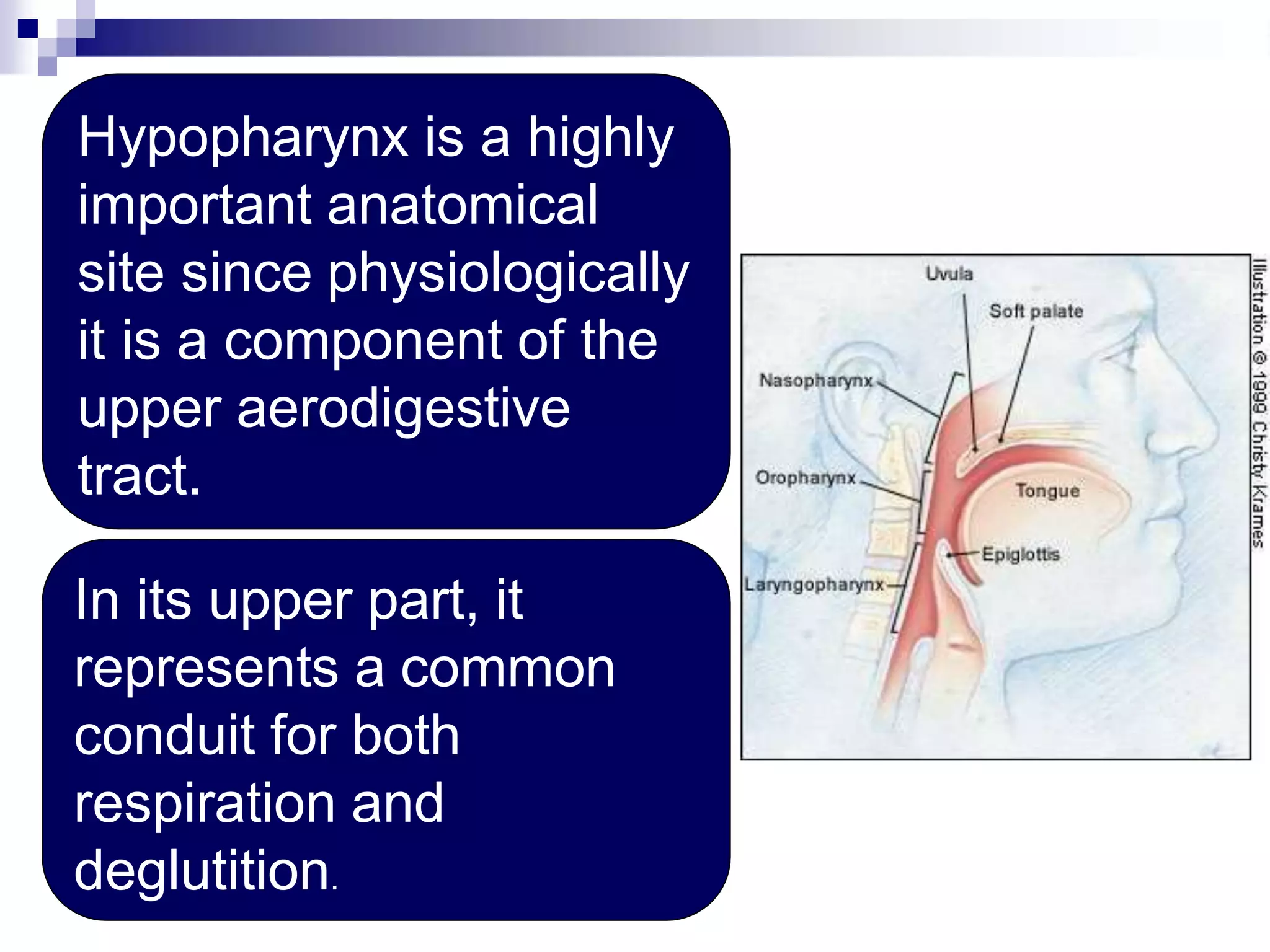
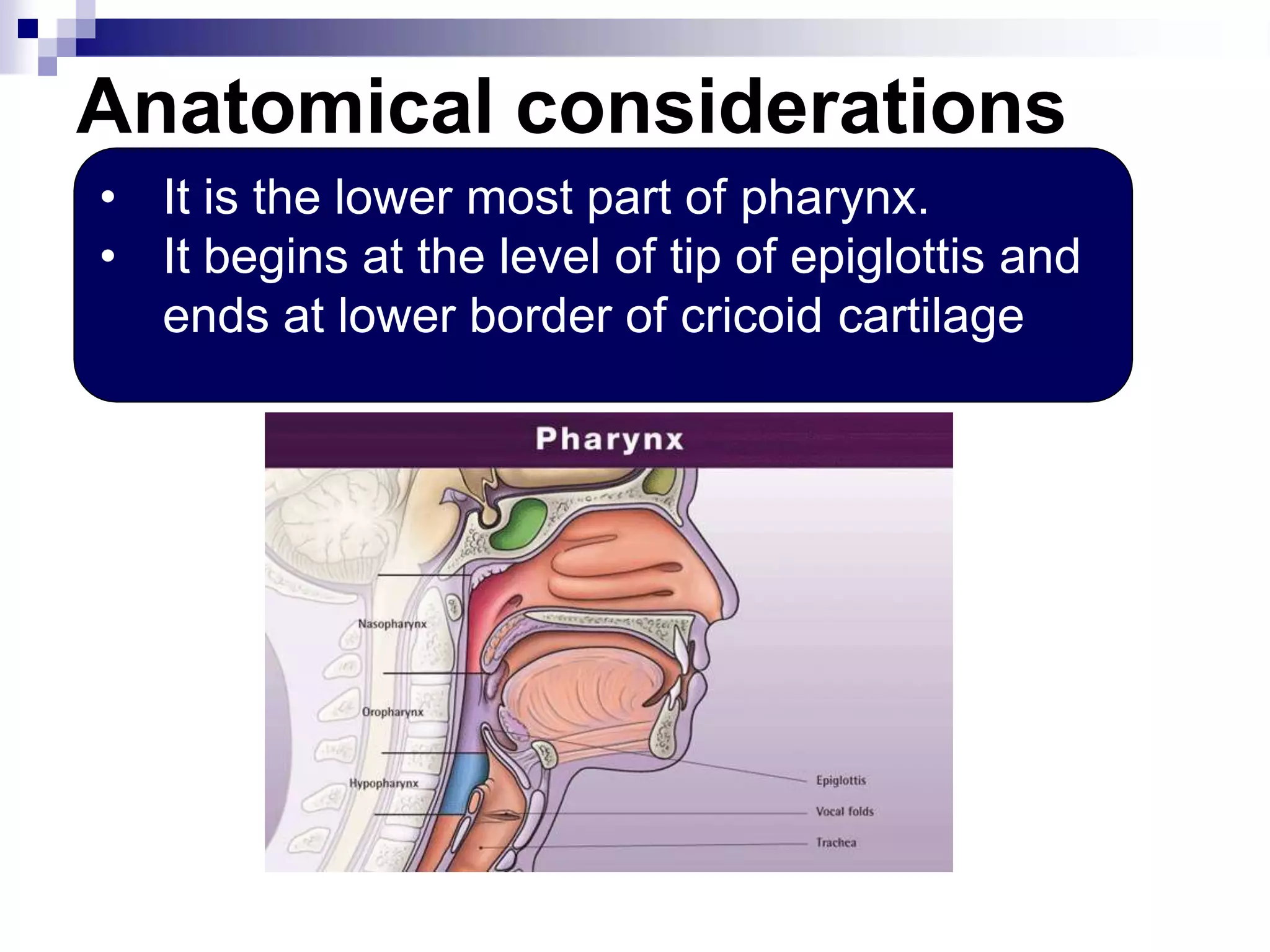
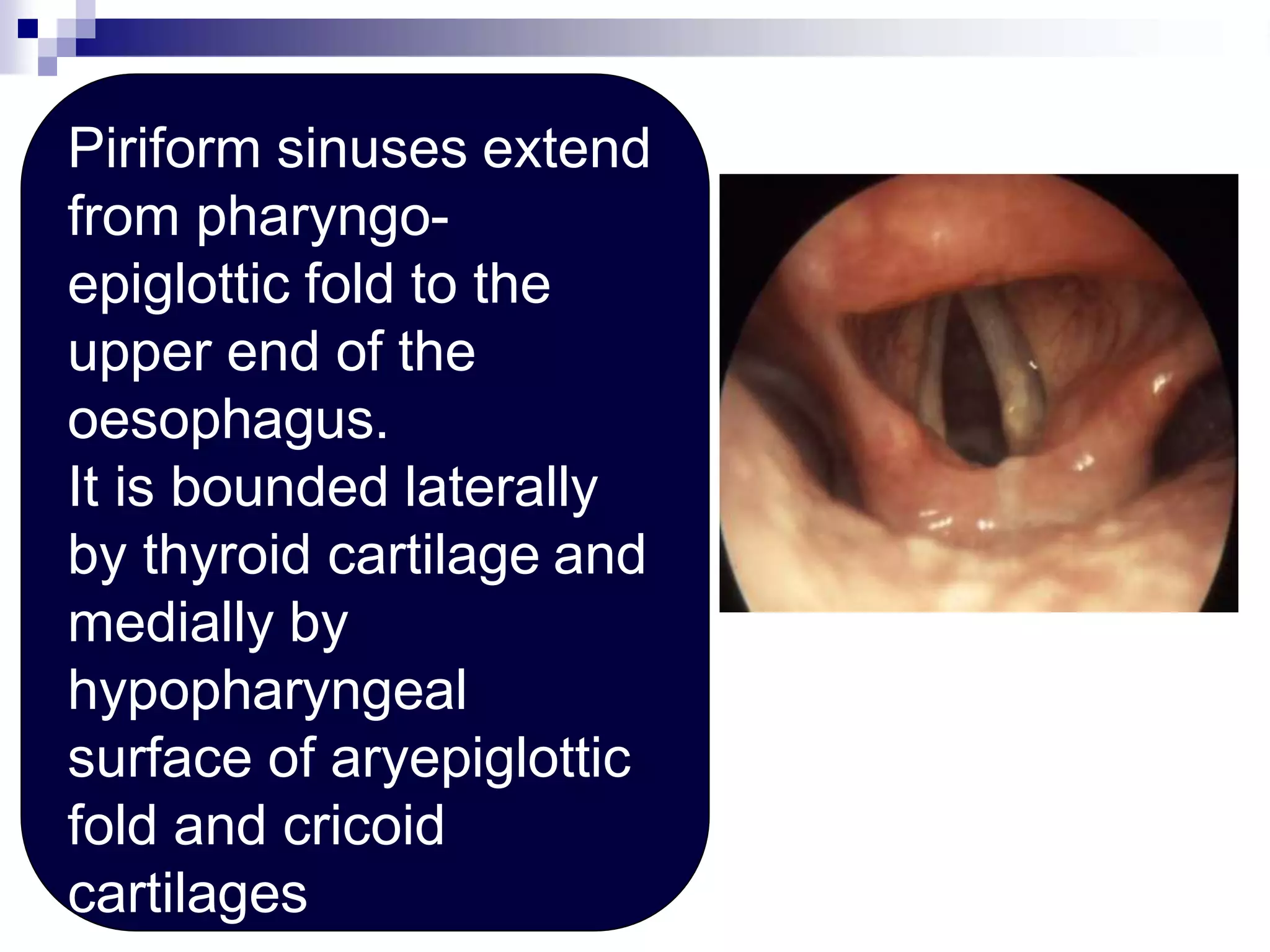
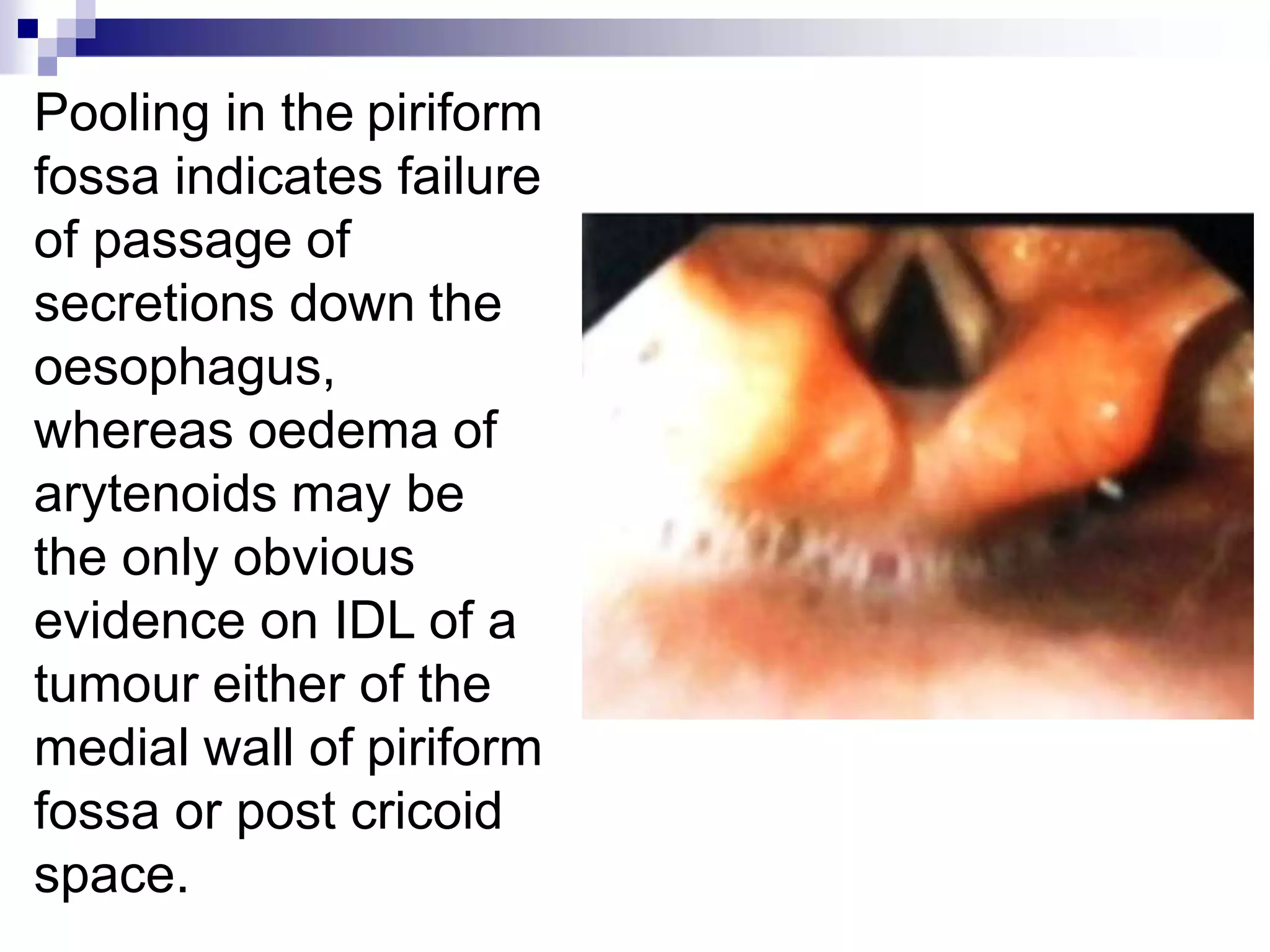
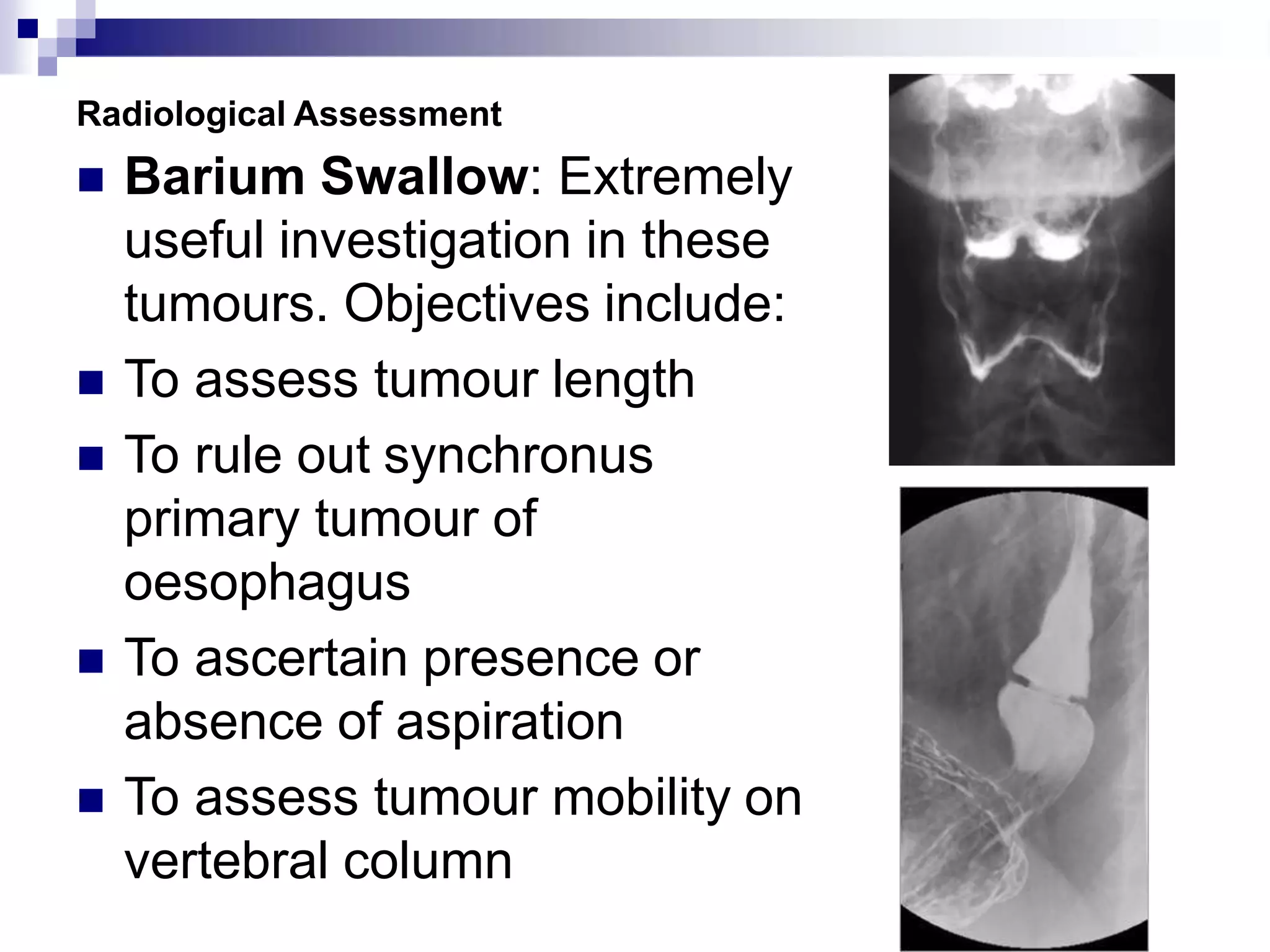
This document discusses carcinoma of the hypopharynx. It begins with an overview of hypopharynx anatomy and notes that tumors in this region often present at an advanced stage. It emphasizes the importance of early and accurate diagnosis, staging, and treatment with curative intent using surgery and postoperative radiotherapy. The document then provides further details on hypopharynx anatomy, symptoms, examination findings, diagnostic evaluations, staging criteria, and various surgical treatment options for hypopharyngeal carcinoma.