Downloaded 401 times
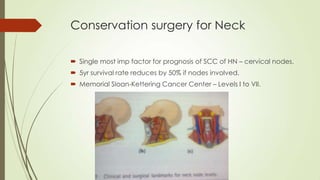
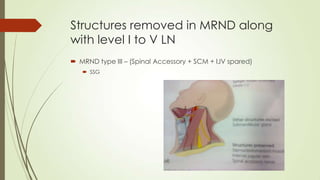



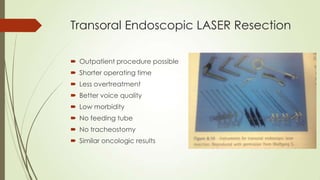




This document discusses principles of conservative surgery for head and neck cancers. It covers selective and comprehensive neck dissection techniques for managing cervical lymph nodes. It describes various open and endoscopic surgical procedures to preserve structure and function for cancers of the larynx and hypopharynx, including vertical partial laryngectomy, supracricoid laryngectomy, and transoral laser resection. Complications and oncologic outcomes of these organ preservation techniques are also discussed.


































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)















