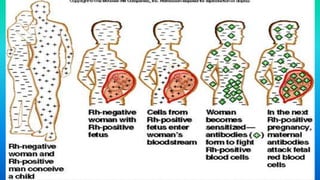
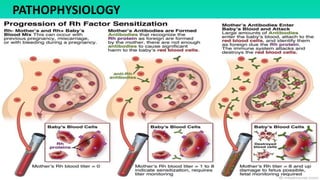
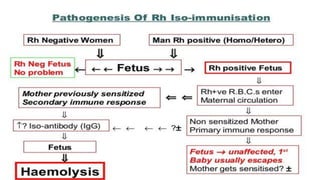
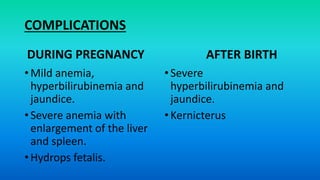
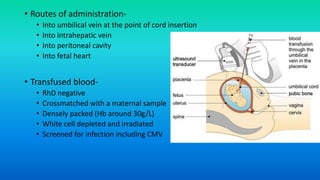
Rh incompatibility occurs when a pregnant woman has Rh-negative blood and her fetus has Rh-positive blood. During pregnancy or delivery, the fetus's Rh-positive blood can enter the mother's bloodstream and cause her to form antibodies. If she has another Rh-positive baby, those antibodies can cross the placenta and destroy the baby's red blood cells, causing anemia or even hydrops fetalis. To prevent Rh disease, Rh-negative mothers are given Rh immunoglobulin injections during and after pregnancy to prevent antibody formation. For affected pregnancies, fetal blood transfusions may be needed to treat severe anemia.