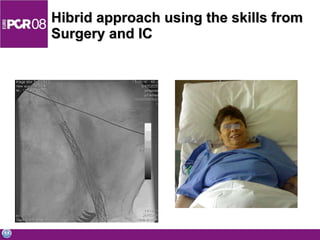
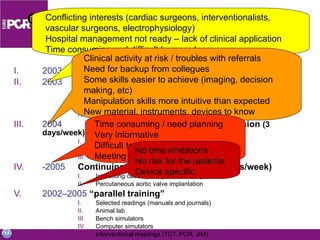
The document discusses the need for cross-training of surgeons and interventional cardiologists in percutaneous heart valve treatment. It states that the procedure requires skills independent of one's base discipline, and that specific training is required. Those undergoing the procedural training should be experienced interventionalists or surgeons. The document then outlines various pathways for acquiring the necessary skills through simulation, proctoring, visiting other centers, and industry-supported opportunities.


























































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




