This document discusses strategies to optimize transcatheter aortic valve replacement (TAVR) programs, including:
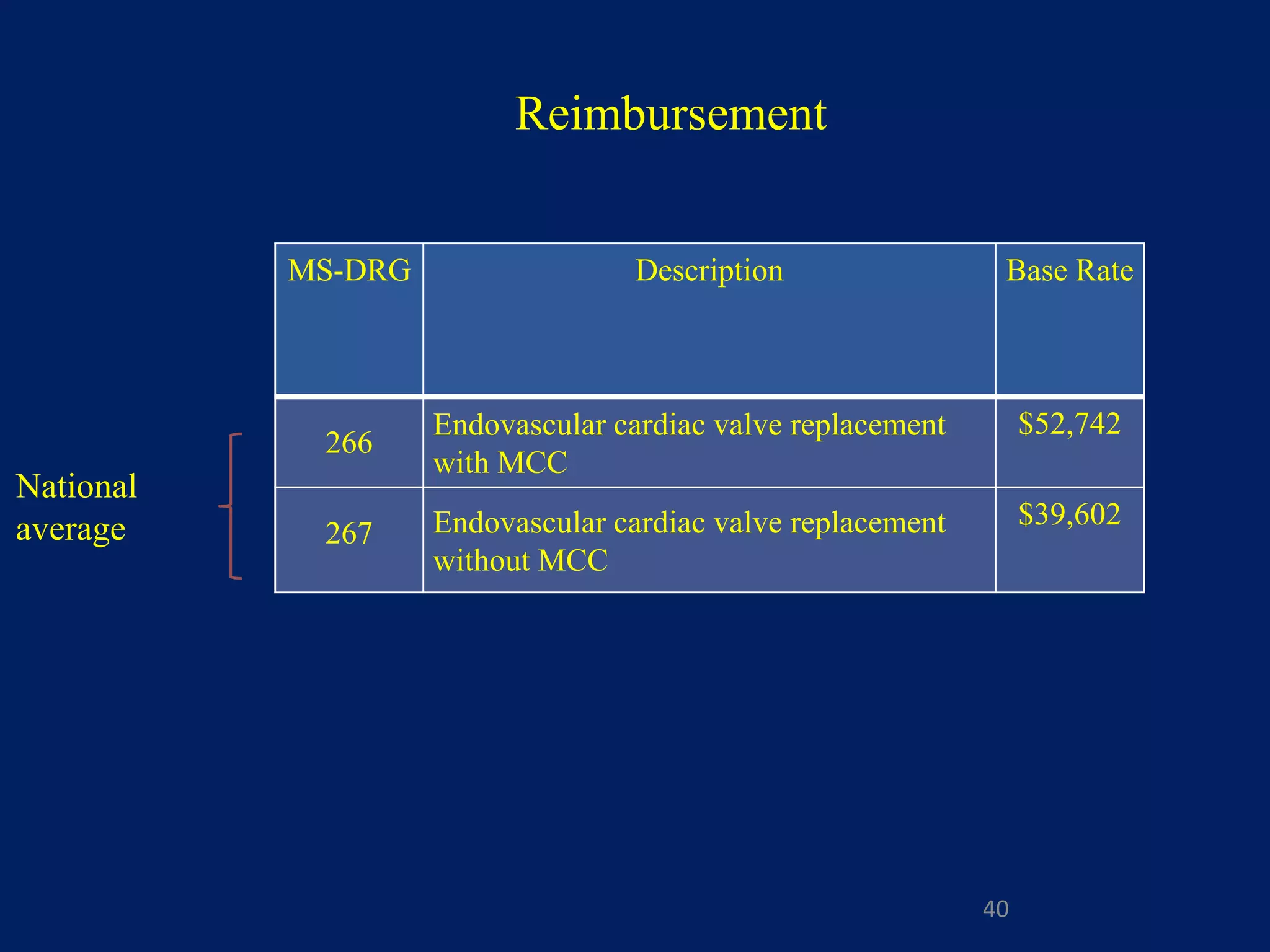
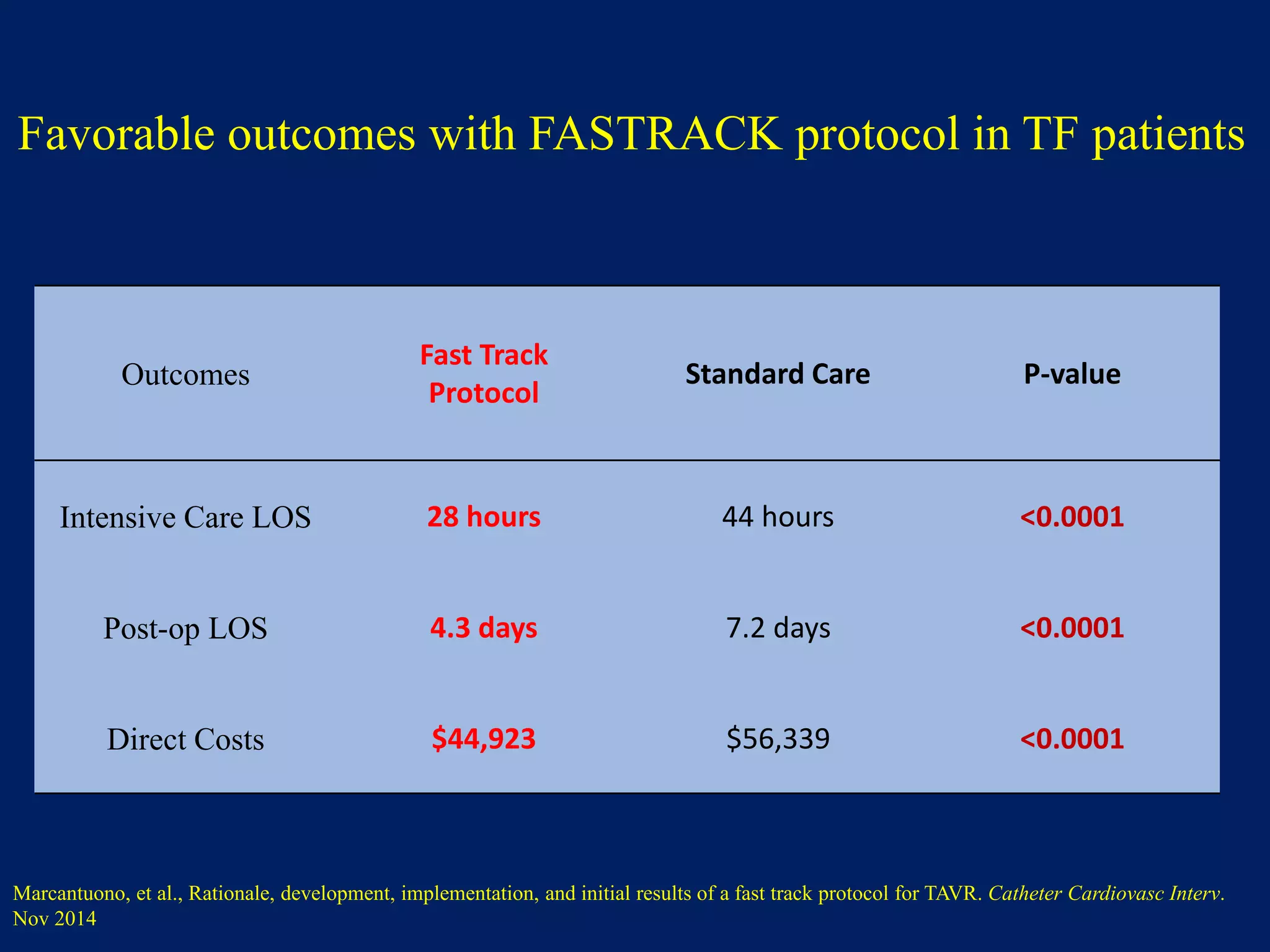
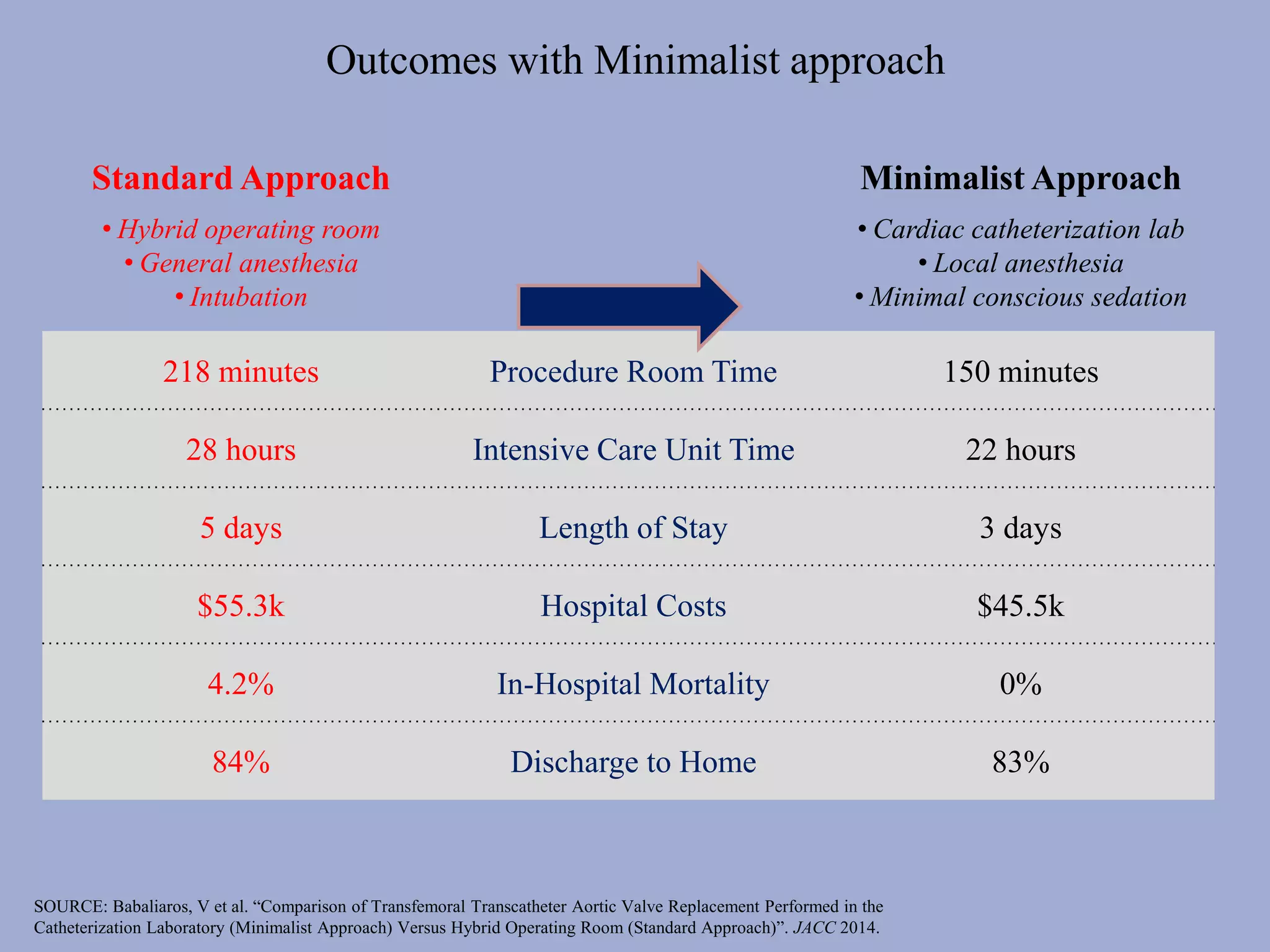
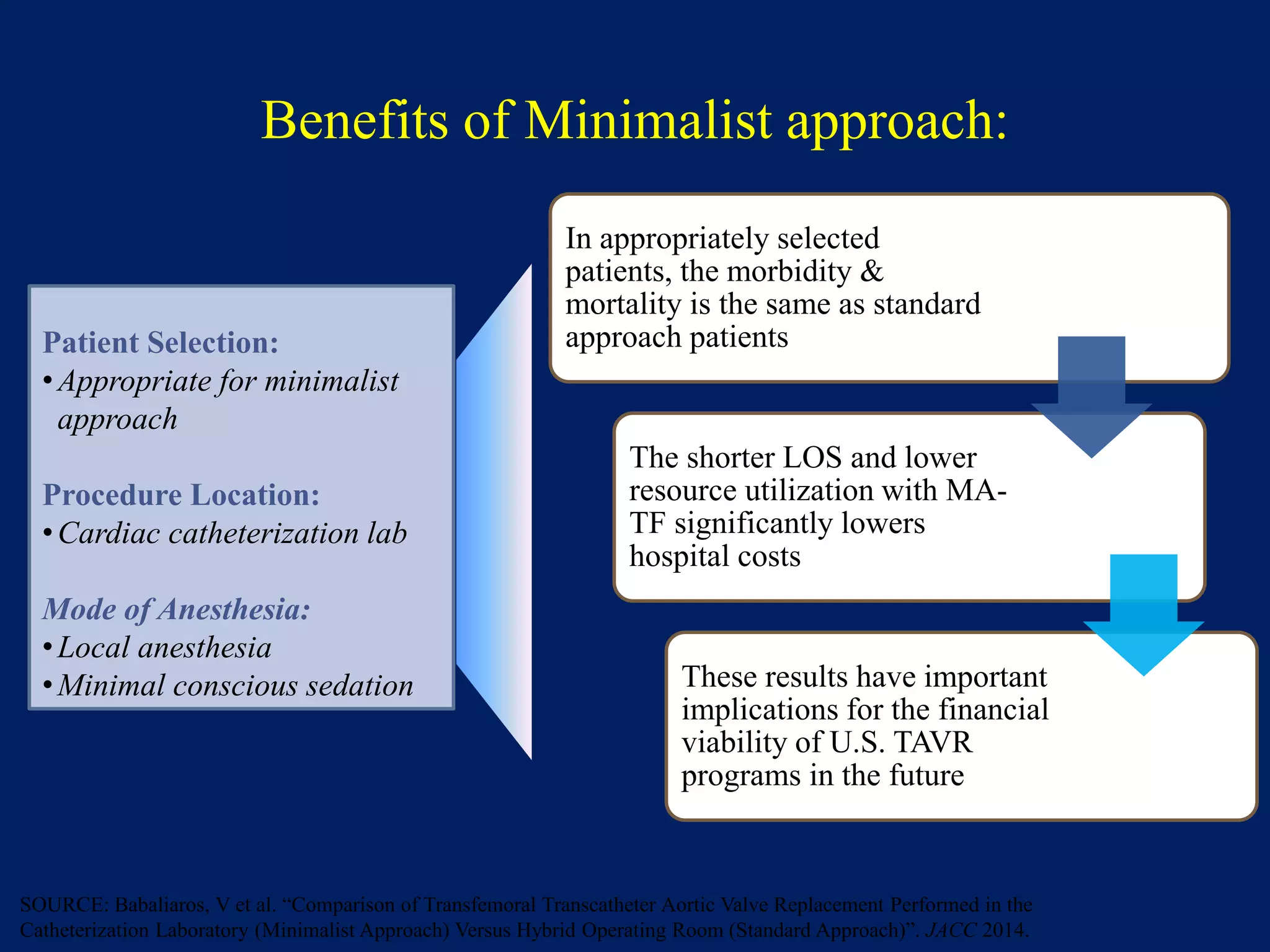
1. Implementing a minimalist approach to TAVR procedures using local anesthesia and conscious sedation in the catheterization lab, rather than general anesthesia in the hybrid operating room, which can reduce procedure time, intensive care unit stay, length of stay, and hospital costs.
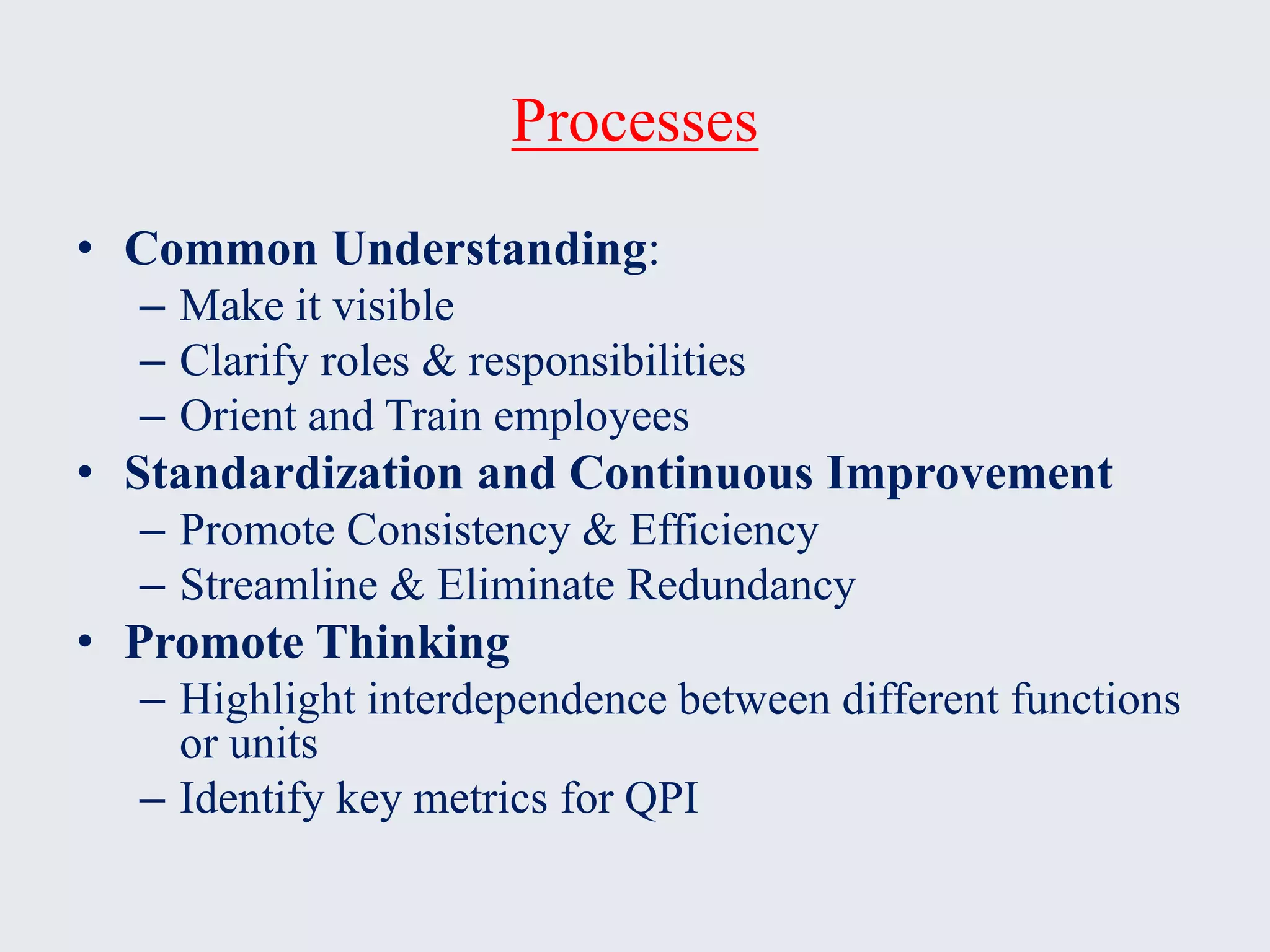
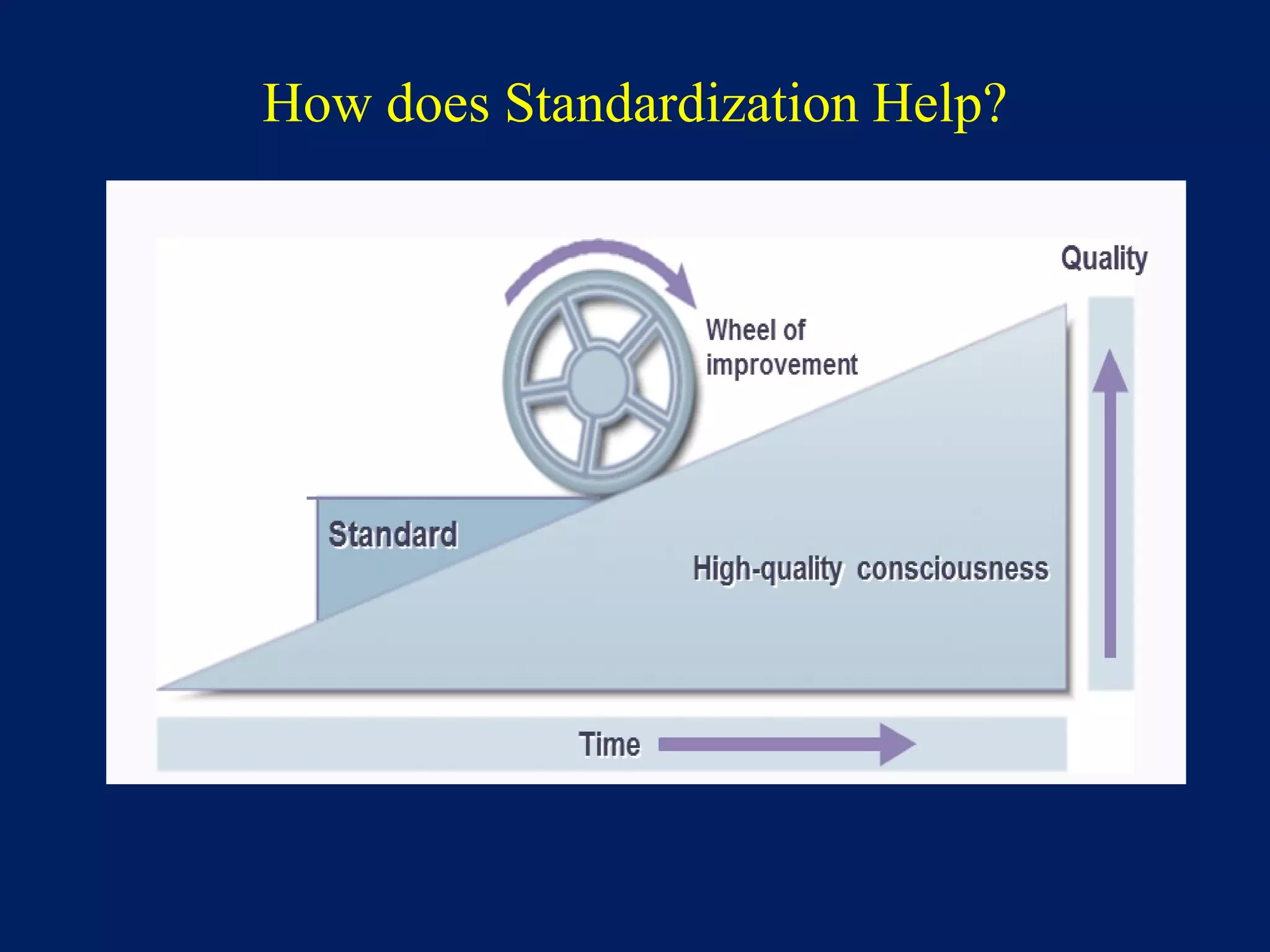
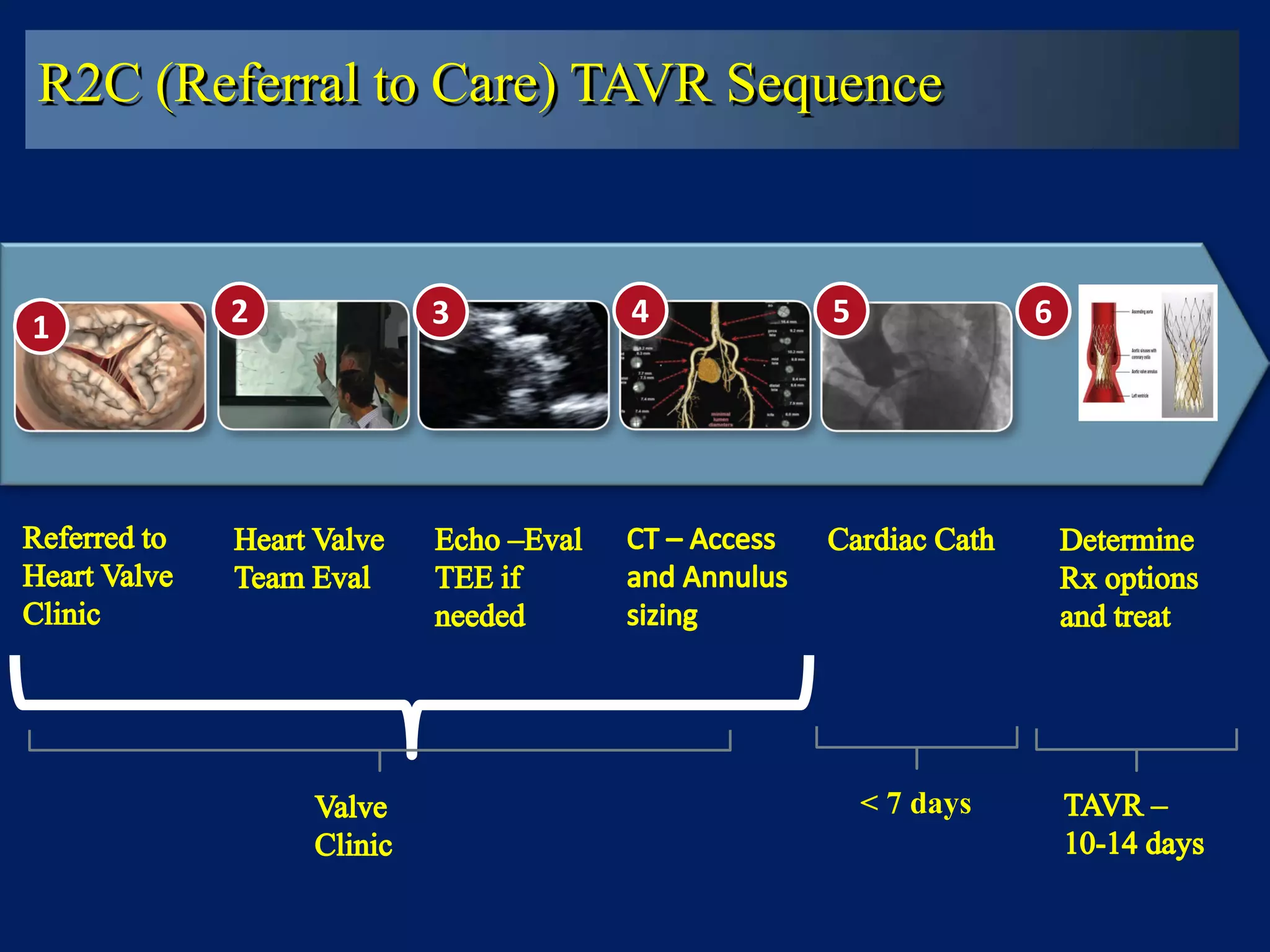
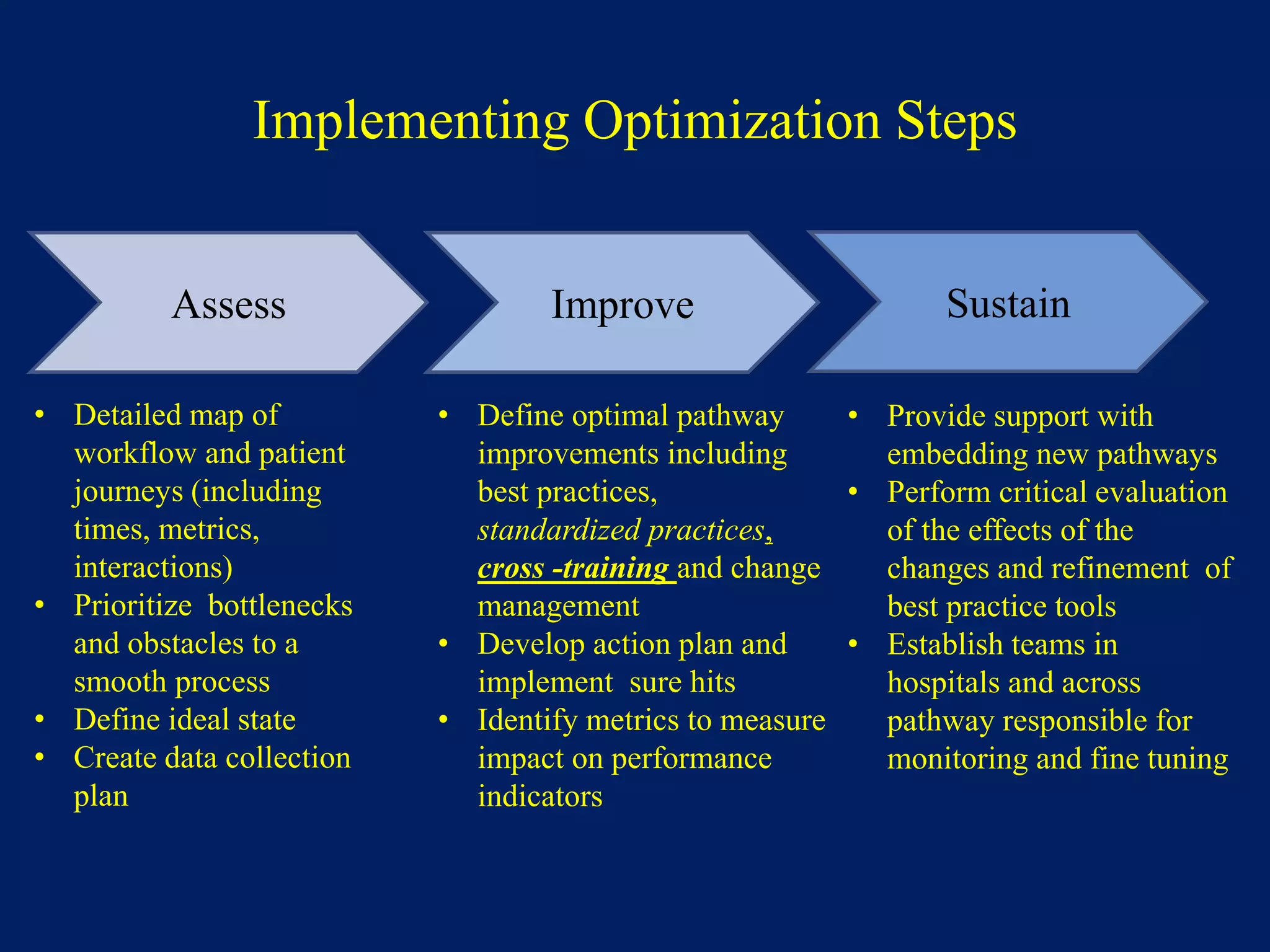
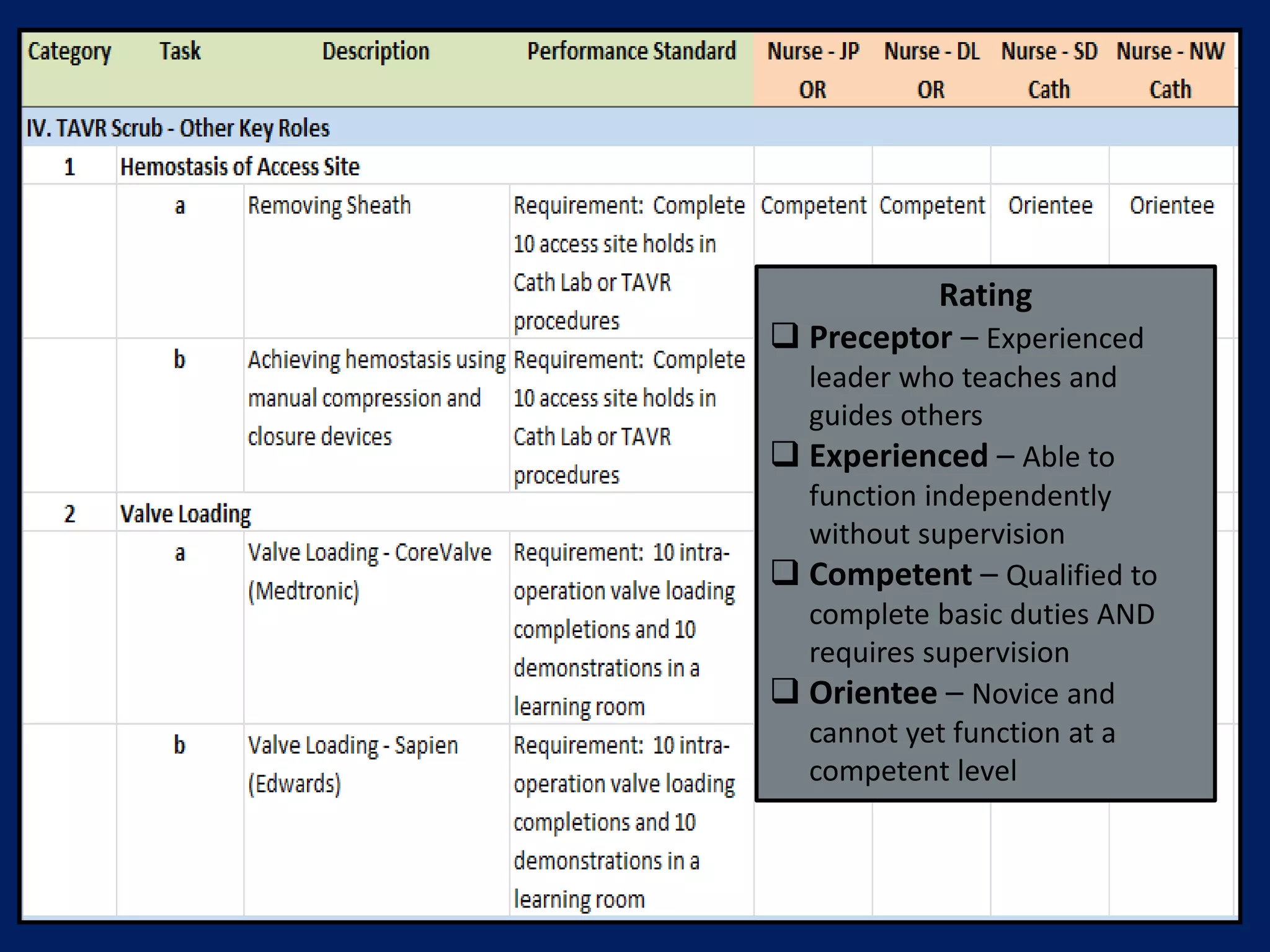
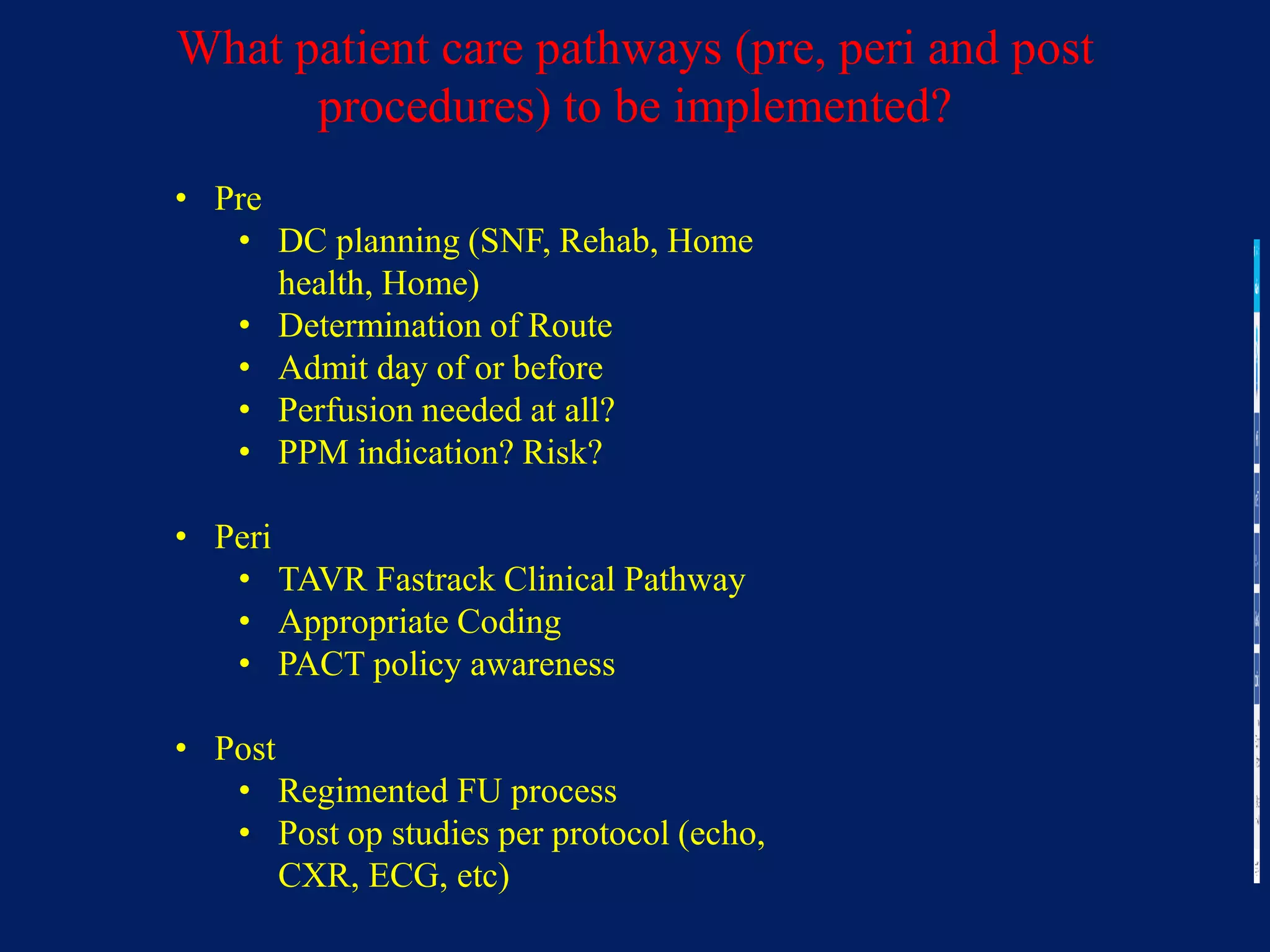
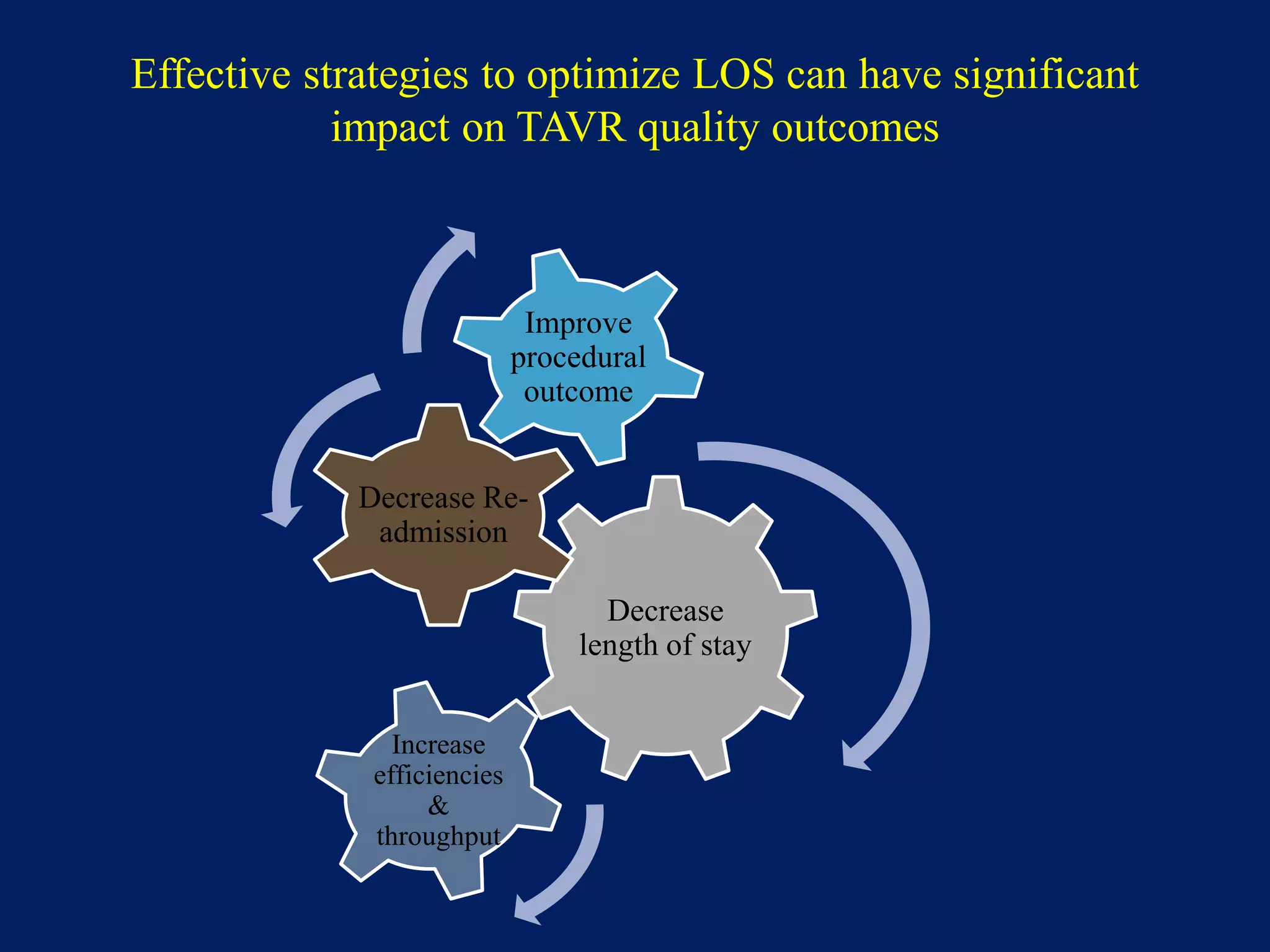
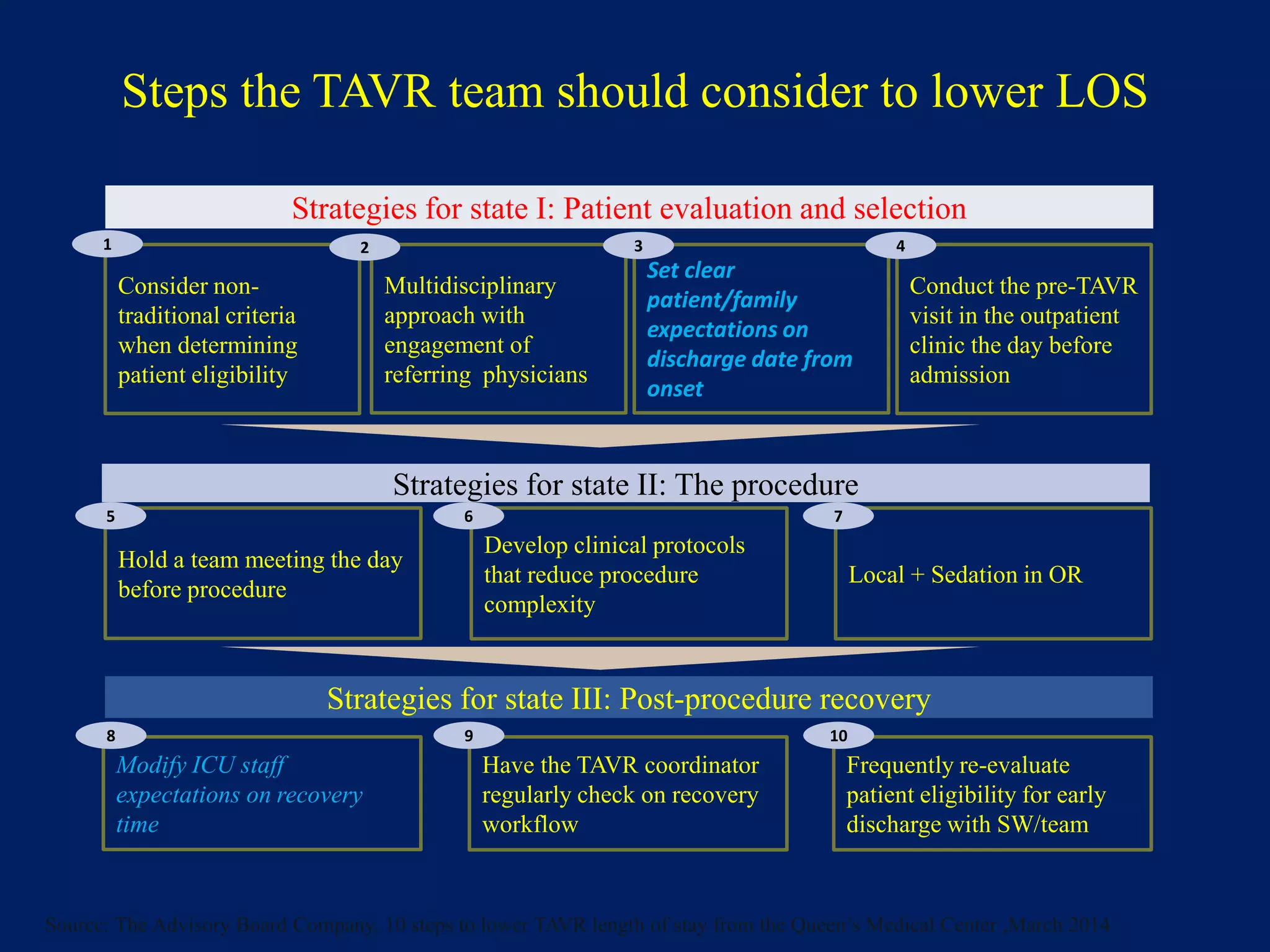
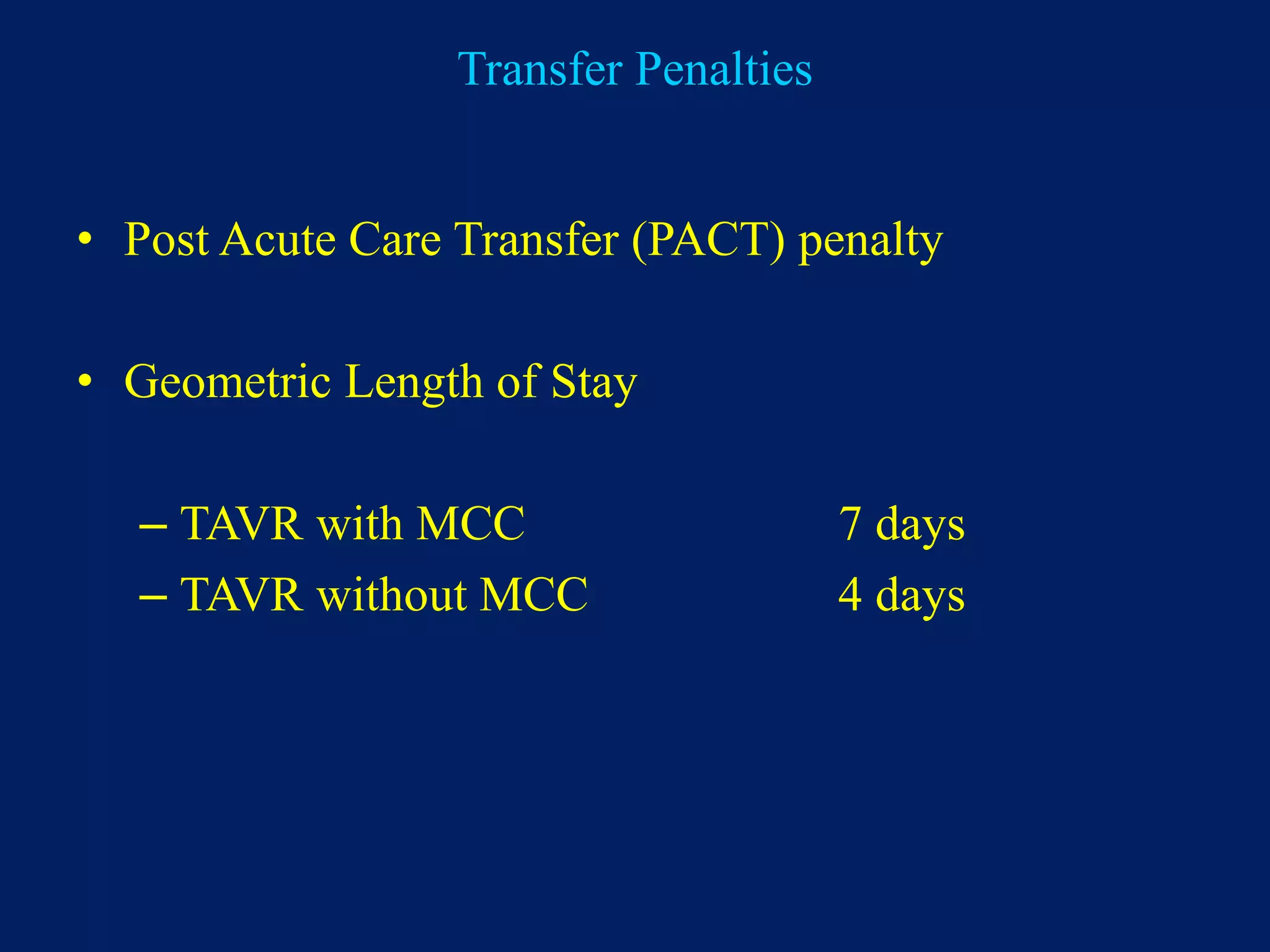
2. Developing standardized clinical pathways and protocols for pre-procedure patient evaluation and selection, the TAVR procedure itself, and post-procedure recovery, in order to decrease length of stay and readmissions while improving outcomes.
3. Considering ways to decrease resource utilization such as reducing hospital staff duplication, streamlining procedure-