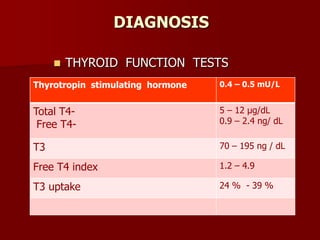
The document discusses hyperthyroidism, detailing the anatomy, physiology, diagnosis, and treatment of thyroid dysfunction. It covers the synthesis and action of thyroid hormones, diagnostic tests, and treatment options including antithyroid drugs, radioactive iodine, and surgery. Additionally, it outlines anesthesia management considerations for patients with thyroid issues, emphasizing the importance of achieving a euthyroid state prior to surgical procedures.

























![Thyroid ppt [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/thyroidpptautosaved-170310134424-thumbnail.jpg?width=640&height=640&fit=bounds)











![THYROID DISORDERS AND ANAESTHESIA.ppt[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/thyroiddisordersandanaesthesia-240826093351-632c8bba-thumbnail.jpg?width=640&height=640&fit=bounds)




















![Anesthesia for thyroid_disease....day_2[1]](https://cdn.slidesharecdn.com/ss_thumbnails/anesthesiaforthyroiddisease-181123090354-thumbnail.jpg?width=640&height=640&fit=bounds)






























