Downloaded 227 times















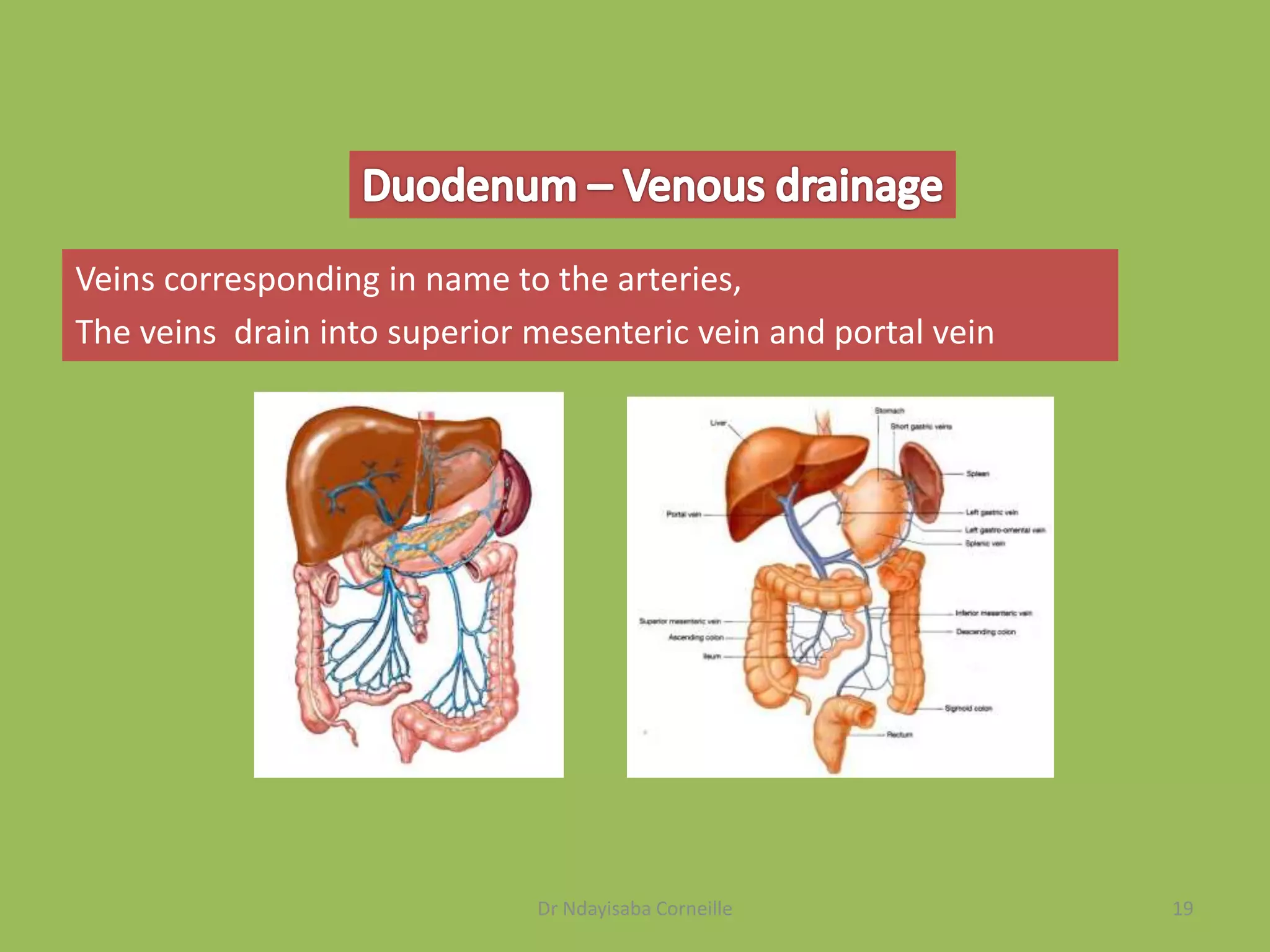


































The document provides a comprehensive overview of the small intestine, detailing its anatomy, histology, and functions. It highlights the specific parts, including the duodenum, jejunum, and ileum, along with their respective roles in digestion and nutrient absorption. Additionally, the document describes vascular supply, nerve innervation, and conditions affecting the small intestine, such as ulcers and Meckel's diverticulum.























































































